
Idioma
Effects of placentophagy in the puerperium: an integrative review
Effects of placentophagy in the puerperium: an integrative review
Efeitos da placentofagia no puerpério: uma revisão integrativa
ABSTRACT
Objective: to analyze the scientific evidence in the health literature on placentophagy and its use as a therapeutic resource to increase lactation and treat postpartum depression. Method: integrative literature review, in the following electronic databases: SCOPUS; EMBASE; MEDLINE via PubMed and Scholar Google, without a time marker. Results: seven articles made up the sample, two randomized studies and one cohort study, which described and analyzed the consumption of placenta capsules versus placebo. Two cross-sectional studies were carried out using questionnaires on the practice of placentophagy and its motivations in a population of women recruited through social networks; and two retrospective cohort studies, which used medical records. Conclusion: the results presented in this review point to a challenge in care practice, which should be guided by informed patient choice and a humanized relationship.
Descriptors: Placenta; Feeding Behavior; Breastfeeding; Postpartum Depression; Postpartum Period; Obstetrics; Autonomy rate.
RESUMO
Objetivo: analisar as evidências científicas da literatura na área de saúde sobre a placentofagia, e sua utilização como um recurso terapêutico para aumentar a lactação e tratar a depressão pós-parto. Método: revisão integrativa da literatura com coleta nas seguintes bases de dados eletrônicas: SCOPUS; EMBASE; MEDLINE via PubMed e Scholar Google, sem marcador temporal. Resultados: sete artigos compuseram a amostra, sendo dois estudos randomizados e um estudo de coorte, o qual descreveu e analisou o consumo da placenta em cápsulas versus placebo. Dois estudos transversais foram realizados por meio da aplicação de questionários sobre a prática da placentofagia e suas motivações em uma população de mulheres recrutadas por meio de redes sociais; e dois estudos coorte retrospectivo, que usou registros médicos. Conclusão: os resultados apresentados nesta revisão apontam para um desafio na prática assistencial, que deve ser guiada pela escolha informada da paciente e o relacionamento humanizado.
Descritores: Placenta; Comportamento Alimentar; Aleitamento Materno; Depressão Pós-Parto; Período Pós-Parto; Obstetrícia; Autonomia
INTRODUCTION
Pregnancy and the puerperium are times when significant physiological, psychological, social, and emotional changes occur in women's lives. These changes can leave women vulnerable to feelings such as sadness and anxiety, which can then trigger mood swings and depression1-2. Worldwide, the proportion of women with postpartum depression reaches 13% in high-income countries and 20% in low-income countries3. In Brazil, around 25% of puerperal women experience depression.4
Recognizing this stage of intense transformations in the construction of motherhood, one of the aspects that can corroborate depression in the puerperium is the breastfeeding period, since this is strongly related to mood swings. For some women, not being able to breastfeed leads to feelings of inability to care for their child, causing suffering and feelings of sadness and low self-esteem. It is known that short breastfeeding periods or interruptions in breastfeeding are associated with higher rates of maternal depression.5
If, on the one hand, stopping or not breastfeeding can lead to postpartum depression, on the other, myths and beliefs that guide lactation can lead to feelings of guilt, anxiety, or confidence among breastfeeding women.6
The United Nations (UN) and the United Nations Children's Fund (UNICEF) recommend exclusive breastfeeding as the ideal food for babies, from the first hour after giving birth until six months of age, due to its benefits for the child's healthy growth and development7. However, it should be emphasized that it is during this period that postpartum depression appears most frequently.8-9
One of the treatments for postpartum depression is the use of antidepressant medication. Among the disadvantages of drug treatment in the postpartum period are the side effects of antidepressants and low adherence to treatment due to maternal fear that the medication will be passed on to the newborn through breast milk, which could have harmful effects.10
In this sense, the search for medicinal treatments and alternative practices that don't interfere with the puerperium has been gaining prominence and new followers, such as placentophagy. This is defined as the practice of consuming the placenta. Although the first scientific research into placentophagy in humans was carried out in the early 1900s11-12 and later in the 195013, the phenomenon of placentophagy gained notoriety through the reports of celebrities who consumed their own placenta believing in its benefits. Since then, more and more health professionals have come across puerperal women requesting their placenta for consumption.
Although placentophagy is becoming more and more common, there are as yet no estimates of its use in Brazil. According to a study conducted in the Pacific Northwest of the United States, 50% of women who gave birth at home and 10% of women who gave birth in birthing centers or hospitals practiced placentophagy, i.e., around two thousand women consume their placentas every year in this area, due to a series of maternal benefits.14
Among the reported benefits of placentophagy are the prevention or reduction of postpartum depression and improved mood in the puerperium, increased lactation, increased energy, and accelerated maternal recovery after childbirth15-16. Placenta can be consumed in various ways, the most common being through capsules prepared after steaming, dehydration, grinding, and encapsulation. Other forms of consumption are: in the form of vitamins, placental alcohol extract, replacing meat in recipes such as lasagna, or even "in natura".17
The limitations in terms of the type and quality of research on placentophagy were observed by several researchers who unanimously reported the need for further scientific research on the subject.14-15,18-20
Thus, given the evidence on the importance of breastfeeding and the impacts of depression in the puerperal period, the growing discussion on placentophagia, as well as the scarcity of studies addressing the subject; the aim of this study is to support health professionals, including obstetric nurses and midwives, in their care practice.
OBJECTIVE
To analyze the scientific evidence in the health literature on placentophagy and its use as a therapeutic resource to increase lactation and treat postpartum depression.
METHOD
This is an integrative review of the literature21, which sought to determine the knowledge on the subject of the study, deepening the knowledge about the objective investigated, in order to identify, analyze, and synthesize the results, making it possible to identify the gaps in knowledge of a phenomenon. It was developed based on the following stages: identification of the topic and selection of the research question; defining the inclusion and exclusion criteria; defining the information to be extracted from the selected studies; careful evaluation of the included studies; interpretation of the results, presentation of the integrative review and the recommendations set out in the PRISMA Statement.22
In formulating the problem, the PICO strategy21,22 was adapted to answer the following guiding question: "Is there any evidence that the practice of placentophagy increases milk production and reduces postpartum depression in women in the puerperium?" We therefore considered: P: women who consumed the placenta; I: practice of placentophagy; C: no comparison; and O: decrease in depression and increase in lactation.20
The inclusion criteria were: primary and complete health papers published in Portuguese, English, and Spanish, with no time frame which answered the guiding question of this study. Duplicate publications, letters to the reader, editorials, theses, dissertations, books, book chapters, newspaper articles, experience reports, reflective studies, systematic or integrative literature reviews, and studies that did not deal with this topic were excluded.
Data was collected in November 2021 and reviewed in September 2023 using the following electronic databases: SCOPUS; EMBASE; MEDLINE/PubMed portal and SCHOLAR GOOGLE. The following keywords were used to extract the articles: placentophagy; eating placenta; breastfeeding, lactogen, and prolactin. No descriptor was found in Decs and Mesh for "placentophagy". The Boolean operators OR and AND were used, considering that the controlled descriptors are standardized terms defined by specialists. The search was assisted by a professional trained in databases.
Due to the access characteristics of the selected databases, strategies combined in different ways were used, with the aim of achieving a broad search, based on the guiding axis of the study question and the established inclusion criteria (Chart 1).
Chart 1 - Descriptors derived from the study question.
|
Database |
Search framework |
|
Embase |
‘placentophagy’/ AND (‘prolactin’/ OR prolactin OR ‘breast feeding’/ OR ‘breast feeding’) |
|
Scopus |
((placentophagia or placentophagy) AND (“breastfeeding” OR prolactin OR lactogen)) |
|
Scholar Google |
"human placentophagy" AND (breastfeeding OR lactogen OR prolactin) |
|
MEDLINE/PubMed |
(((placentophagy) OR (eating placenta) OR (placenta ingestion) OR (placentophagia))) AND (breastfeeding) |
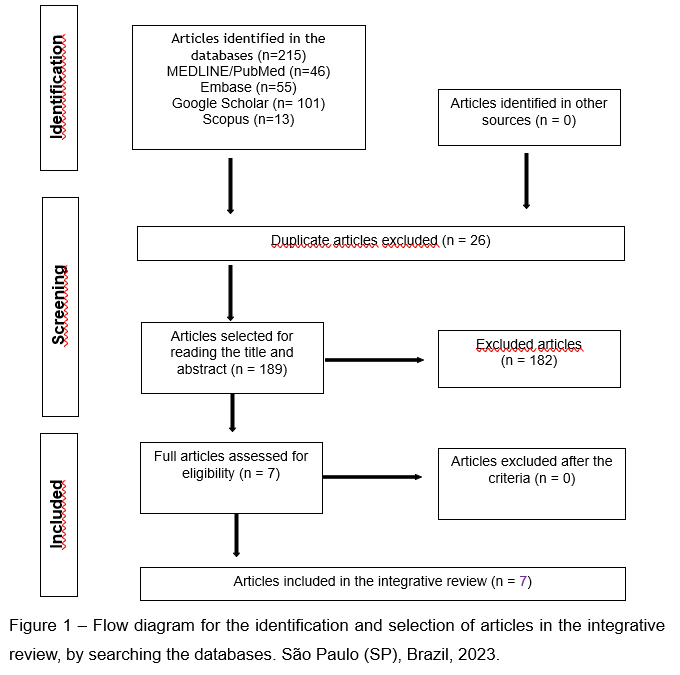
Based on the analysis carried out, a total of 215 studies were identified in the databases, distributed as follows: MEDLINE/PubMed (46), EMBASE (55), Scholar Google (101), and SCOPUS (13). Of these, 26 duplicate articles were excluded, leaving 189 articles that were analyzed by title and abstract, many of which were blog reports. After this, 182 articles were excluded because they did not meet the inclusion criteria. As a result of this process, seven articles met the eligibility criteria, as illustrated in figure 1.
To collect and analyze the data from the seven articles, we used a table containing: studies selected according to authors, year of publication, country of origin, level of evidence, objective, method/sample, and main results. The level of evidence of the studies was assessed using the Oxford classification.23
Once the analysis was complete, a synthesis of the important elements was carried out in order to portray the theme and process of the review. The data was interpreted critically and impartially to provide possible explanations for the results found, regardless of whether they were convergent or conflicting, based on the available literature.
RESULTS
Seven articles made up the sample of this integrative review, as shown in Table 2, according to the general characteristics: author, year, country, language, and level of evidence.
Chart 2 - Characterization of the articles included in the integrative review according to title, year, country, language, and level of evidence. São Paulo (SP), Brazil, 2021.
|
ID(a) |
Author |
Year of publication |
Country |
Language |
Level of Evidence |
|
1 |
Selander et al. (19) |
2013 |
USA |
English |
2C |
|
2 |
Benyshek et al. (24) |
2018 |
USA |
English |
2B |
|
3 |
Stanley et al. (25) |
2018 |
Canada |
English |
2C |
|
4 |
Young et al. (26) |
2018 |
USA |
English |
1B |
|
5 |
Young et al. (27) |
2019 |
USA |
English |
1B |
|
6 |
Morris et al. (28) |
2019 |
Canada |
English |
2B |
|
7 |
Benyshek |
2023 |
EUA |
Inglês |
2B |
Note: ID(a) = article identification number.
The articles included in this review were published in English and the following countries: the United States of America19,24,26,27,29 and Canada 25,28. Of the seven articles, one study was published in 2013, three in 2018, and two in 2019, and one in 2023. From a methodological and objective point of view, three studies described and analyzed the consumption of placenta capsules versus placebo, two of which were randomized26-27 and one a cohort study28; two cross-sectional studies19,25 evaluated the practice of placentophagy and its motivations in a population of women recruited through social networks; and two retrospective cohort study used medical records24,29 to evaluate the motivations and experiences associated with placenta consumption.
Two studies are classified as level 1B26-27, three studies as level 2B24,28,29, and two studies with level of evidence 2C19,25. Table 3 summarizes the articles included in the review, including author/year/country, level of evidence, objective, method/sample, results, and outcomes.
Chart 3 - Characterization of the selected studies according to title, objective, method/sample, and main results.
|
Title |
Objective |
Method/Sample |
Main results |
|
Human maternal placentophagy: A survey of self-reported motivations and experiences associated with placenta consumption. |
To examine the demographic data, form of consumption, motivations, and experiences of women who have practiced placentophagy. |
Cross-sectional study carried out using an online questionnaire with women who had practiced placentophagy. Recruitment through social media. Questionnaires with open and closed questions (n = 189). Between October and November 2010. |
Reasons for placentophagy (304 answers): mood improvement: 34%; restore/balance metabolism: 8%; increase in lactation: 7%; recovery from childbirth: 7%. Form of consumption: encapsulated: 80%. Positive experiences reported: improved mood: 40%; increased energy: 26%; improved lactation: 15%; relief from bleeding: 7%. Negative experiences reported: none: 69%; unpleasant taste/smell: 7%; headache: 4%; other: 20%. Positive experiences (Likert scale): very positive: 75%; positive: 20%; slightly positive: 4%; not positive: 1%. |
|
Placentophagy among women planning community births the United States: Frequency, rationale, and associated neonatal outcomes. |
(a) To describe the demographic characteristics associated with placentophagy; (b) To describe the forms of consumption and the main reasons for consuming the placenta. (c) To evaluate neonatal outcomes among women who consumed and did not consume their placentas. |
Data collected from the Midwives Alliance of North America Statistics (MANA Stats) registry: n = 23,242 Consumed the placenta: 7,162 (30.8%). Duration: May/2015 to December/2016. |
Reasons for consumption: improvement of mood/prevention of "postpartum depression": 73.10%; nutritional support (treatment or prevention of anemia): 14.20%; improvement of lactation: 4.85%; increase in energy: 4.51%; reduction of postpartum bleeding: 1.30%. Preparation methods: dehydrated (raw) and encapsulated: 48.4%; cooked/steamed and then encapsulated: 36.6%; raw (alone or as a smoothie, etc): 9.00%. Neonatal outcomes: there was no association between placenta consumption and the three adverse outcomes assessed in the study (admission to the NICU in the first six weeks, neonatal hospitalization in the first six weeks, or neonatal / infant death in the first six weeks). |
|
Understanding Placentophagy |
Description of demographic data and assessment of the knowledge, attitudes, and beliefs of women during pregnancy and the postpartum period related to placentophagy. |
Cross-sectional study carried out using an online questionnaire and an online discussion group (mixed method). Online questionnaire with 21 close-ended and open-ended questions with short answers. Discussion groups with recruitment on social networks n = 1214 / 271 consumed placenta. Duration: June 28th to July 31st, 2017. Period of discussions: July to October 2017. |
Reasons for consumption (n = 1,088): - Midwife recommendation: 9.4%; - Family or friend recommendation: 8.9%; - Recommendation from doula: 8.3%; - Curiosity to try: 20.2%; - Belief that the benefits outweigh the potential risks: 21.4%; - Interest in alternative and/or natural health practices: 21.3%. Reasons for not consuming (n = 1.079): - Not having heard of it: 5.9% Belief that the risks outweigh the benefits: 10.0%; - Aversion to the idea of eating placenta: 30.0%; Perceived benefits (n = 1,030): - Increased energy / decreased fatigue: 44.7%; - Improved lactation: 41.4%; - Decreased postpartum depression: 50.4%; - Increase in iron stores: 50.6%; - Decreased vaginal bleeding after childbirth: 22.8%; - Faster uterine evacuation: 22.7%; - Pain relief: 9.3%. Risk / Negative effects (n = 1.030): - Unpleasant taste/smell: 67.3%; - Headache: 6.1%; - Infection: 45.0%; - Blood clots: 2.9%; - Exposure to heavy metals and/or toxins: 22.1%; - Decreased lactation: 4.7% Online discussions: the most cited topics were postpartum depression, hormone restoration, lactation, preparation and handling, interaction with the health system, and friends as information resources. |
|
Placentophagy’s effects on mood, bonding, and fatigue: A pilot trial, part. 2 |
To investigate and compare measures of depressive symptoms, fatigue, and maternal bonding in the postpartum period in women who ingested their own dehydrated and encapsulated placentas with these measures in women who ingested a placebo supplement at the beginning of the postpartum period. |
Randomized, double-blind, placebo-controlled study. Eligible 36. Placenta group 17. Placebo group 19. Analyzed (n = 27). Placenta group 12. Placebo group 15. Data collection: standardized questionnaires at four meetings with researchers (during the 36th week of pregnancy, within 96 hours of delivery, between five and seven days of delivery, and during the third week postpartum (between days 21 and 27 postpartum)) Consumption of the placenta: capsules after the 2nd meeting with the research team until day 21 postpartum. |
Anxiety, stress, maternal bonding, and fatigue were not affected by placenta consumption. Sleep quality: there was no difference improvement in sleep quality in the placebo group between meetings two and three and meetings two and four. The study showed no benefits from placentophagy. |
|
Ingestion of Steamed and Dehydrated Placenta Capsules does not affect postpartum plasma prolactin levels or neonatal weight gain: results from a randomized, double-blind, placebo-controlled pilot study |
To evaluate the effects of placentophagy on plasma prolactin concentration and neonatal weight gain. |
See item 4 |
Plasma prolactin levels in both groups decreased over the study period, with no difference in plasma prolactin concentration after placenta supplementation (F = 0.856, P = 0.36). Neonatal weight gain: there was no statistical difference between the groups in terms of newborn weight (F = 2.344, P = 0.10) or neonatal weight gain (F = 0.669, P = 0.42). |
|
A matched cohort study of postpartum placentophagy in women with a history of mood disorders: no evidence for impact on mood, energy, vitamin B12 levels, or lactation |
To empirically investigate the effect of postpartum placentophagy on maternal mood, energy, micronutrients, and lactation. |
Retrospective cohort study with case matching n = 138 (100% of the sample with a history of mood disorder); Questionnaires at three time points postpartum (one to two weeks; one to two months; and three to four months postpartum). Simple recording: consumption or non-consumption. Lactation deficiency was measured by the use of domperidone (lactation inducer). Pairing: 4 x 1 n = 28 (placentophagia) n = 110 (non-placentophagia). |
There were no differences in the indicators of postpartum depression (P = 0.282) and energy (P = 0,389). Use of domperidone: - Placentophagia = 4 (14.29%); - Non-placentophagia = 17 (15.45%).
There were no differences between the groups in symptoms of depression, energy levels, or domperidone use. |
|
Comparison of placenta consumers’ and nonconsumers’ postpartum depression screening results using EPDS in US community birth settings (n=6038): a propensity score analysis |
To compare the PPD screening scores of placenta consumers and non-consumers in a community birth setting, using propensity score matching to address the anticipated extensive confounding. |
Data from the "Midwives Alliance of North America Statistics" (MANA Stats) registry between 2016 and 2018. (n=6,038) Compared PPD screening scores measured by the Edinburgh Postpartum Depression Scale (EPDS). Paired analysis of individuals who consumed placenta with those who did not (demographics, pregnancy characteristics and history of mental health problems) Placentophagic group (n=1,876) and non-placentophagic group (n=1,876). Created logistic regression propensity scores based on commonly cited EPDS cut-off values (≥11; ≥13) for probable PPD. |
In the non-matched and unadjusted analysis, placentophagia was associated with an increased risk of PPD. In the matched sample, 9.9% of placentophagic women reported EPDS≥11, compared to 8.4% of women who did not (5.5% and 4.8%, respectively, EPDS≥13 or higher). After controlling for more than 90 variables (including previous mental health challenges) in the combined and adjusted analysis, placentophagia was associated with an increased risk of PPD of between 15 and 20%, depending on the cut-off point published in the EPDS used. Numerous sensitivity analyses did not alter this overall finding. |
Two of the articles with the highest level of evidence selected for the review were part of the same pilot clinical trial, which randomized 36 patients, with a loss of nine patients during the study period. In this study, 17 patients who consumed the placenta in encapsulated form and 19 patients who consumed placebo were analyzed. Data collection using questionnaires and laboratory blood samples from the participants was carried out by the researchers at four meetings between the 36th week of pregnancy and the third week postpartum (between days 21 and 27 postpartum). The intake of placenta capsules began after the second meeting and lasted until the end of the study, totaling 21 days of supplementation.26-27
The authors reported the outcome concerning mood swings26, by evaluating standardized questionnaires, and the other concerning lactation and breastfeeding, by collecting laboratory analysis and neonate weight data.27
One of the studies included in the integrative review was a retrospective analysis of a prospective cohort of 365 patients who had psychiatric disorders before pregnancy. In this analysis, the authors matched one case in which placenta was consumed with four control cases (without placenta consumption) and collected data on mood disorders using standardized questionnaires. The breastfeeding variable was measured indirectly through reports of taking medication that stimulates lactation (domperidone).28
Two studies analyzed data from a North American birth registry called "Midwives Alliance of North America Statistics" (MANA Stats), containing more than 23,000 women, 30.8% of whom reported placentophagy. In one of them, the authors reported demographic data, trying to identify the factors involved in placentophagy, as well as the reasons for consumption, the method of preparation for consumption, and the analysis of neonatal outcomes of women who consumed and did not consume placenta in the postpartum period24. In another study, the authors carried out a paired analysis of two groups (placentophagy and non-placentophagy) comparing the results of the EPDS.29
Two of the articles with the highest level of evidence selected for the review were part of the same pilot clinical trial, which randomized 36 patients, with a loss of nine patients during the study period. In this study, 17 patients who consumed the placenta in encapsulated form and 19 patients who consumed placebo were analyzed. Data collection using questionnaires and laboratory blood samples from the participants was carried out by the researchers at four meetings during the period between the 36th week of pregnancy and the third week postpartum (between days 21 and 27 postpartum). The intake of placenta capsules began after the second meeting and lasted until the end of the study, totaling 21 days of supplementation.26,27
The authors reported the outcome concerning mood swings(26), through the evaluation of standardized questionnaires, and the other concerning lactation and breastfeeding, through the collection of laboratory analysis and neonate weight data.27
One of the studies included in the integrative review was a retrospective analysis of a prospective cohort of 365 patients with psychiatric disorders before pregnancy. In this analysis, the authors matched one case in which placenta was consumed with four control cases (without placenta consumption) and collected data on mood disorders using standardized questionnaires. The breastfeeding variable was measured indirectly by reporting the use of medication that stimulates lactation (domperidone).28
Finally, two articles described the epidemiological profile of women who were identified on social networks and who answered online questionnaires. These articles also described the demographic profile, beliefs, and motivations, ways of consuming placenta, and positive and negative experiences of placentophagy.19,25
DISCUSSION
This review aimed to explore the literature in search of studies on the benefits of placentophagy for treating symptoms of postpartum depression and increasing lactation. Seven studies answered the guiding question of this review, demonstrating that the phenomenon has been little explored scientifically in recent years, in contrast to the growing interest in this practice in several countries, including Brazil.
Women are consuming their placenta in the postpartum period in various forms (encapsulated, cooked, and raw), believing that this practice may have a therapeutic role and bring health benefits such as preventing postpartum depression, increasing lactation and energy, replenishing nutrients lost in childbirth, and reducing pain and uterine bleeding more quickly. In the United States, where the subject is widely covered by the media, a study consecutively analyzed 23,242 planned births in communities with midwives (obstetric centers/local birthing centers or home births) and found that 30.8% (7,162) of these women consumed postpartum placenta.
In the same study, the motivations most cited by these women for this practice were: mood improvement/prevention of postpartum depression (73.1%), nutritional support or prevention of anemia (14.2%), improved lactation (4.8%), and improved energy (4.5%).24
In the study carried out by Selander19, the experiences with placentophagy were positive for most of the practitioners (very positive: 75%; positive: 20%; slightly positive: 4%), and 98% of the women reported that they would do it again19. In studies where patients self-reported the benefits, there was an improvement in mood of between 40% and 50.4% and an improvement in lactation of between 15% and 41.4%.19,25
Regarding postpartum depression, one of the studies 25 shows that, although women are aware that there are no scientifically proven benefits, they prefer to adopt the practice of placentophagy in order to prevent PPD, thinking of avoiding traditional pharmacological treatments. In this study, among the motivations cited by the participants, 21.3% reported an interest in natural health practices, and 20.2% felt motivated after having heard/read about the subject.
Although exploratory studies based on self-reports show results in favor of the practice, qualitative studies that assess outcomes in a standardized way present data that do not show differences between women who practice placentophagy or not.
Two publications originated from the same randomized trial and evaluated the outcomes of placentophagy concerning mood changes and postpartum depression, and concerning lactation.26,27 Regarding depressive symptoms, there was no difference between women who consumed placenta or not, although the authors noted a trend towards a reduction in depressive symptoms in the placenta supplementation group during the first week postpartum. However, the results did not show any statistically significant differences between the groups at the end of the evaluation, which evened out over the days.26
With regard to lactation, placenta supplementation did not alter maternal serum prolactin levels in the postpartum period or neonatal weight gain.27 Likewise, in a cross-sectional study that analyzed neonatal outcomes (admission to the neonatal ICU, neonatal hospitalization, or neonatal/infant death in the first six weeks), no differences were found between the newborns of mothers who consumed placenta and those whose mothers did not.24
Placentophagia was also evaluated in comparison to symptoms of postpartum depression and lactation in a retrospective cohort study of a database of 365 women with diagnoses of psychiatric disorders. The study showed that there was no difference in symptoms of depression, nor was there any difference between the groups in terms of the use of domperidone as a lactation inducer.28
In a 2023 publication, the authors carried out a retrospective study of a database of North American home birth records ("Midwives Alliance of North America Statistics" - MANA Stats). his was a matched analysis of cases and controls by propensity score that included 90 variables, comparing the EPDS in the group that consumed the placenta with the group that did not. 1,876 cases were matched in each group, and the results showed that 9.9% of placentophagic women reported EPDS≥11, compared to 8.4% of women who did not (5.5% and 4.8%, respectively for EPDS≥13). Even adopting two EPDS cut-off levels, the results showed a higher risk of PPD, 15 and 20% respectively, in women who consumed the placenta.29
CONCLUSION
The results presented in this review point to a challenge in care practice, which should be guided by patient safety and a humanized relationship.
According to the literature, the practice of placentophagy is linked to feelings of improvement, which are not corroborated by clinical studies. Therefore, the answer to the guiding question of the study is that there is no clinical evidence that the practice of placentophagy increases milk production or decreases postpartum depression in women in the puerperium.
It is therefore up to health professionals to advise pregnant women/society about the lack of scientific evidence that placenta ingestion increases lactation and reduces postpartum depression, and about the possible risks involved. Placentophagy should therefore be a woman's informed choice, after being informed about the issue, and it is not up to the health professional to indicate whether or not the woman should eat the placenta.
CONTRIBUTIONS
All the authors contributed equally to the conception of the research project, the collection, analysis, and discussion of the data, as well as the writing and critical revision of the content with their intellectual contribution and approval of the study's final version.
CONFLICTS OF INTERESTS
Nothing to report.
FUNDING
Funding agencies: CNPQ, CAPES, Foundations, etc.
REFERENCES
- Arrais AR, Araujo TCCF. Depressão pós-parto: uma revisão sobre fatores de risco e de proteção. Psic Saúde Doenças. 2017 Oct;18(3):828–45. DOI: https://dx.doi.org/10.15309/17psd180316
- Ghaedrahmati M, Kazemi A, Kheirabadi G, Ebrahimi A, Bahrami M. Postpartum depression risk factors: a narrative review. J Educ Health Promot. 2017 Aug; 6:60. DOI: https://doi.org/10.4103/jehp.jehp_9_16
- Meltzer-Brody S, Howard LM, Bergink V, Vigod S, Jones I, Olsen TM, et al. Postpartum psychiatric disorders. Nat Rev Dis Primers. 2018 Apr; 4:18022. DOI: https://doi.org/10.1038/nrdp.2018.22
- Theme Filha MM, Ayers S, Gama SGN, Leal MC. Factors associated with postpartum depressive symptomatology in Brazil: the birth in Brazil national research study, 2011/2012. J Affect Disord. 2016 Apr;194:159–67. DOI: https://doi.org/10.1016/j.jad.2016.01.020
- Dias CC, Figueiredo B. Breastfeeding and depression: a systematic review of the literature. J Affect Disord. 2015 Jan;171:142–54. DOI: https://doi.org/10.1016/j.jad.2014.09.022
- Marques ES, Cotta RMM, Priore SE. Mitos e crenças sobre o aleitamento materno. Ciên Saúde Colet. 2011 May;16(5):2461–8. DOI : https://doi.org/10.1590/S1413-81232011000500015
- World Health Organization. Expert consultation on the optimal duration of exclusive breastfeeding [Internet]. Geneva: World Health Organization; 2001 [cited 2022 Aug 12]. Available from: https://www.who.int/nutrition/publications/optimal_duration_of_exc_bfeeding_report_eng.pdf
- Nam JY, Choi Y, Kim J, Cho KH, Park EC. The synergistic effect of breastfeeding discontinuation and cesarean section delivery on postpartum depression: a nationwide population-based cohort study in Korea. J Affect Disord. 2017 Aug; 218:53–8. DOI: https://doi.org/10.1016/j.jad.2017.04.048
- Figueiredo B, Canário C, Field T. Breastfeeding is negatively affected by prenatal depression and reduces postpartum depression. Psychol Med. 2014 Apr;44(5):927–36. DOI: https://doi.org/10.1017/S0033291713001530
- O'Hara MW, Engeldinger J. Treatment of postpartum depression: recommendations for the clinician. Clin Obstet Gynecol. 2018 Sep;61(3):604–14. DOI: https://doi.org/10.1097/GRF.0000000000000353
- Hammett FS, McNeile LG. Concerning the effect of ingested placenta on the growth-promoting properties of human milk. Science. 1917a Oct;46(1188):345–6. DOI: https://doi.org/10.1126/science.46.1188.345
- Hammett FS, McNeile LG. The effect of the ingestion of desiccated placenta on the variations in the composition of human milk during the first eleven days after parturition. J Biol Chem [Internet]. 1917b [cited 2022 Aug 12];30(1):145–53. Available from: https://www.sciencedirect.com/science/article/pii/S002192581886759X
- Soyková-Pachnerová E, Brutar V, Golová B, Zvolská E. Placenta as a lactagagon. Gynaecologia. 1954;138(6):617–27. DOI: https://doi.org/10.1159/000308239
- Cole M. Placenta medicine as a galactogogue: tradition or trend? Clin Lact [Internet]. 2014 [cited 2022 Aug 12];5(4):116–22. Available from: http://dx.doi.org/10.1891/2158-0782.5.4.116
- Marraccini ME, Gorman KS. Exploring placentophagy in humans: problems and recommendations. J Midwifery Womens Health. 2015 Jul/Aug;60(4):371-7. DOI: https://doi.org/10.1111/jmwh.12309
- Hayes EH. Consumption of the placenta in the postpartum period. J Obstet Gynecol Neonatal Nurs. 2016 Jan/Feb;45(1):78-89. DOI: https://doi.org/10.1016/j.jogn.2015.10.008
- Farr A, Chervenak FA, McCullough LB, Baergen RN, Grünebaum A. Human placentophagy: a review. Am J Obstet Gynecol. 2018 Apr;218(4):401.e1-401.e11. DOI: https://doi.org/10.1016/j.ajog.2017.08.016
- Young SM, Benyshek DC. In search of human placentophagy: a cross-cultural survey of human placenta consumption, disposal practices, and cultural beliefs. Ecol Food Nutr. 2010 Nov/Dec;49(6):467-84. DOI: https://doi.org/10.1080/03670244.2010.524106
- Selander J, Cantor A, Young SM, Benyshek DC. Human maternal placentophagy: a survey of self-reported motivations and experiences associated with placenta consumption. Ecol Food Nutr. 2013;52(2):93-115. DOI: http://dx.doi.org/10.1080/03670244.2012.719356
- Coyle CW, Hulse KE, Wisner KL, Driscoll KE, Clark CT. Placentophagy: therapeutic miracle or myth? Arch Womens Ment Health. 2015 Oct;18(5):673-80. DOI: https://doi.org/10.1007/s00737-015-0538-8
- Sousa LM, Marques-Vieira CM, Severino SS, Antunes AV. Metodologia de revisão integrativa da literatura em enfermagem. Rev Investigação Enferm [Internet]. 2017 [ cited 2023 Dec 29]; 2(21): 17-26. Available from : https://www.researchgate.net/publication/321319742_Metodologia_de_Revisao_Integrativa_da_Literatura_em_Enfermagem
- Page MJ, Mckenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Multrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372(71). DOI: 10.1186/s13643-021-01626-4
- Oxford Centre for Evidence Based Medicine. Levels of evidence: grades of recommendation [Internet]. Oxford: CEBM, 2009 [cited 2022 Aug 12]. Available from: http://www.cebm.net/index.aspx?o=1025
- Benyshek DC, Cheney M, Brown JLM, Bovbjerg ML. Placentophagy among women planning community births the United States: frequency, rationale, and associated neonatal outcomes. Birth. 2018 Dec;45(4):459-68. DOI: http://doi.org/10.1111/birt.12354
- Stanley C, Baillargeon A, Selk A. Understanding placentophagy. J Obstet Gynecol Neonatal Nurs. 2019 Jan;48(1):37-49. DOI: https://doi.org/10.1016/j.jon.2018.10.002
- Young SM, Gryder LK, Cross C, Zava D, Kimball DW, Benyshek DC. Placentophagy’s effects on mood, bonding, and fatigue: a pilot trial, part. 2. Women Birth. 2018 Aug;31(4):e258-71. DOI: https://doi.org/10.1016/j.wombi.2017.11.004
- Young SM, Gryder LK, Cross CL, Zava D, Norris W, Benyshek D. Ingestion of Steamed and Dehydrated Placenta Capsules does not affect postpartum plasma prolactin levels or neonatal weight gain: results from a randomized, double-bind, placebo-controlled pilot study. J Midwifery Womens Health. 2019 Jul;64(4):443-50. DOI: https://doi.org/10.1111/jmwh.12955
- Morris E, Slomp C, Hippman C, Inglis A, Carrion P, Batallones R, et al. A matched cohort study of postpartum placentophagy in women with a history of mood disorders: no evidence for impact on mood, energy, vitamin B12 levels, or lactation. J Obstet Gynaecol Can. 2019 Sep;41(9):1330-7. DOI: https://doi.org/10.1016/j.jogc.2019.02.004
- Benyshek DC, Bovbjerg ML, Cheyney M. Comparison of placenta consumer´s and nom-consumer´s postpartum depression screening results using EPDS in US community birth settings (n=6038): a propensity score analysis. BMC Pregnancy Childbirth. 2023; 23(1):534. DOI: https://doi.org/10.1186/s12884-023-05852-7
Correspondence
Fabiana Lopes Pereira Santana
Email: fabianalps@usp.br
Copyright© 2024 Revista de Enfermagem UFPE on line/REUOL.
This is an open-access article distributed under the CC BY 4.0 Creative Commons Attribution-ShareAlike 4.0 International License, which allows others to distribute, remix, adapt, and create from your work, even for commercial purposes, as long as they credit you for the original creation. It is recommended to maximize the dissemination and use of licensed materials.
 Português (Brasil)
Português (Brasil)  English
English  Español (España)
Español (España) 



















