
Idioma
Quality of life of people affected by leprosy in a highly endemic municipality in Maranhão, Brazil
Carneiro CRN, de Aquino DMC, Monteiro EMLM, Figueiredo IA, Coutinho NPS.
INTRODUCTION
Leprosy is a chronic, infectious disease caused by the bacillus Mycobacterium leprae. It can infect numerous individuals (high infectivity), although few falls ill (low pathogenicity)1. It profoundly alters people's living conditions and, when not treated correctly, can evolve into physical alterations, changing appearance and causing severe limitations2.
The sequelae generated by leprosy are conditions that permanently interfere in the lives of those affected, compromising their daily activities and their Quality of Life (QoL). The Degree of Physical Incapacity (GIF) is responsible for the most significant consequences of the disease, directly affecting productivity in working life, daily activities, and interpersonal relationships. It can also trigger psychosocial disorders and a drop in the QoL of people with the disease, causing social, economic, and psychological damage3.
According to the World Health Organization's Quality of Life Assessment (WHOQOL) Group, QOL can be defined as the individual's perception of their position in life in the context of the culture and value systems in which they live, as well as about their goals, expectations, standards, and concerns4. As such, it is a subjective, complex, and multidimensional concept, encompassing aspects that involve physical and mental health, degree of dependence, personal and social relationships, beliefs and values, and the characteristics of the environment in which the person lives5. QoL is related to the satisfaction of the most basic needs, such as food, access to drinking water, housing, work, education, health, and leisure, fundamental elements that contribute to the comfort, well-being, and individual and collective fulfillment of the human being6.
In 2021, 106 countries reported a total of 140,594 new cases of the disease worldwide to the WHO. In this context, the detection rate of new cases increased by 10.2% compared to 2020, underscoring the urgent need for action. India was the country that registered the latest cases, around 53.6% of the global total. There were 19,826 (14.1%) reported cases in the Americas region, of which 18,318 (92.4%) occurred in Brazil. Brazil thus ranks second among the countries with the highest number of cases globally, followed by Indonesia. The countries that reported the newest cases of leprosy were India, Brazil, and Indonesia, corresponding to 74.5% of the total world7.
Leprosy is on the list of global diseases included as neglected since it is prevalent in conditions of poverty and contributes to maintaining social inequality, representing a significant obstacle for developing countries8.
In March 2020, the WHO declared a pandemic of the new coronavirus, SARS-CoV-2 (Severe Acute Respiratory Syndrome Coronavirus 2), which causes COVID-19 infection. This pandemic has created difficulties for new diagnoses and treatment of leprosy patients, contributing to underreporting and the worse prognosis of cases in Brazil and worldwide9.
Analysis of preliminary data for 2022 shows that Brazil has diagnosed 14,962 new cases of leprosy. Among the states with the highest number of new cases in the general population is Maranhão, with 1,860 cases, followed by Mato Grosso, Pernambuco, Bahia, and Pará, with more than a thousand cases in each Federative Unit (FU)10.
Maranhão is one of the states with a high incidence and prevalence of leprosy11. In 2021, it reached a general detection number of 1,941 cases and a detection rate of 27.13/100,000 inhabitants. However, with the reduction observed in the country due to the COVID-19 pandemic, it is still considered a state of highly high endemicity12. Within this context is the municipality of Pinheiro, which, in the same period, had an annual detection rate in the general population of 23.8/100,000 inhabitants, in line with Maranhão13.
Due to the magnitude of leprosy and its incapacitating power, this disease has become the focus of public health campaigns, as it significantly affects people of working age3.
The Global Leprosy Strategy 2021-2030 represents a significant departure from previous approaches to tackling leprosy on a global scale. While past strategies have made strides in reducing the global leprosy burden, the new plan sets a bold long-term goal: zero leprosies, zero infection and disease, zero disability, zero stigmas, and discrimination14. This ambitious goal should inspire and motivate us to redouble our efforts in interrupting transmission and achieving zero autochthonous cases.
The National Strategy for Tackling Leprosy in Brazil, for the period 2023-2030, presents the vision of a country without leprosy, where the strategic plan is aligned with the international commitments of the WHO and the United Nations (UN). The general objectives for reducing the burden of the disease remain and, as targets, the document provides for reducing the rate of new cases in children under 15, reducing the absolute number of new cases with degree of physical disability 2 (GIF 2) at diagnosis and acting on 100% of complaints about discriminatory practices in leprosy registered through the ombudsman services of the Unified Health System (SUS)10.
The stigma associated with leprosy and discrimination against people affected by the disease challenges early identification and timely completion of treatment. Patients still suffer from social exclusion, depression, and loss of family income because of the disease15.
Given leprosy's multidimensionality, it is essential to assess the quality of life of patients affected by the disease, identify its influence on diverse aspects of the individual, and thus add new concepts to comprehensive care actions for patients12.
This study is relevant in this context as it presents latest information from a period after the COVID-19 pandemic.
OBJECTIVE
To analyze the quality of life of people affected by leprosy in a highly endemic municipality in Maranhão.
METHOD
This is an observational cross-sectional epidemiological study, whose data were collected in the Basic Health Units of the municipality of Pinheiro, located in the northern mesoregion of the state16. Maranhão is made up of 19 health regions (Açailândia, Bacabal, Balsas, Barra do Corda, Caxias, Chapadinha, Codó, Imperatriz, Itapecuru Mirim, Pedreiras, Pinheiro, Presidente Dutra, Rosário, Santa Inês, São João dos Patos, São Luís, Timon, Viana and Zé Doca)16, Pinheiro is considered the micro-region of Baixada Maranhense, with the municipalities of Palmeirândia, Bequimão and Presidente Sarney bordering it, with an estimated population of 84. One hundred sixty inhabitants, a territorial area of 1,512,969 km², and a Human Development Index (HDI) of 0.63717.
The municipality has a health care network made up of two hospitals (one regional and the other in the maternal and child network), a Medical Specialties Center, a Psychosocial Care Center (CAPS, in Portuguese), a Clinical Analysis Laboratory, a Testing and Counseling Center (TCC), an Advanced Mobile Emergency Service (SAMU, in Portuguese) and Family Health Units (17 Family Health Strategy Teams)18. The level of endemicity for leprosy is considered extremely high in the region13. The Leprosy Control Program is implemented in all the FHSs and operates decentralized.
The study included all leprosy cases living in the municipality of Pinheiro-MA, Brazil, aged 18 or over, notified on the Notifiable Diseases Information System (SINAN) between January and December 2022, who were being treated or monitored at the municipality's health units. We excluded those who, after two attempts to collect data, did not show up at the health service (11 cases), were not located (four cases), or were transferred (one case). The intentional non-probabilistic sample consisted of 18 cases (n = 18), corresponding to 53% of the cases notified in 2022.
Data was collected from June 2022 to January 2023 using the following instruments: the Leprosy Cases form, containing sociodemographic, clinical, and epidemiological data; the Simplified Neurological Assessment form (ANS, in Portuguese)19; and the DLQI-BRA20. The study variables included sociodemographic information (gender, color/race, schooling, and family income), clinical information on the disease (operational classification, degree of physical disability, history of leprosy in the family, and length of illness), DLQI-BRA scores and impaired quality of life. The time of illness was considered the period between the onset of the first signs and symptoms reported by the participant and the date of diagnosis.
When the patient went to the health unit, identified by their appointment card/return for follow-up treatment, they were approached for the survey, and the information was collected directly from the participants through the medical records and the SINAN notification form. Because they are self-reported, some information provided during data collection may present response bias. Selection bias is also present in the study, either due to the selective loss of the sample through excluded cases or diagnostic bias.
Data collection began after the research had been explained to the participants, who formally agreed to it by signing the Informed Consent Form (ICF). For illiterate people, consent was obtained by including their fingerprints after clarification. The activities strictly followed the health measures established to control the COVID-19-21 pandemic.
The information was entered into Microsoft Excel® software and analyzed using Epi-Info, version 7 (CDC-Atlanta).
Descriptive statistics were used to analyze sociodemographic, clinical, and quality-of-life variables. Quality of life was assessed using the DLQI-BRA. The DLQI-BRA questionnaire comprises ten questions, each with four answers scored from 0 to 3, covering the last week of the patient's life. The sum of these scores is calculated as the total DLQI points. The scores range from 0 (no impact on quality of life) to 30 (highest level of impact). The sum of the answers makes it possible to analyze the data according to the intervals 0-1 = no effect on the patient's life; 2-5 = small effect on the patient's life; 6-10 = moderate impact on the patient's life; 11-20 = significant effect on the patient's life; 21-30 = massive effect on the patient's life.
The DLQI-BRA results were grouped according to “quality of life score” to check which sociodemographic and clinical variables most frequently compromised quality of life.
The study followed the ethical assumptions of research involving human beings, based on Resolution 466/12 of the National Health Council (CNS), and was submitted to the Research Ethics Committee (CEP) of the University Hospital of the Federal University of Maranhão (UFMA) on November 26, 2020, according to Consubstantiated Opinion No. 4.422.963. It was also resubmitted for approval on August 5, 2022, under new Opinion No. 5.565.810 and Certificate of Submission and Ethical Appraisal (CAAE) No. 29278620.4.0000.5086.
RESULTS
The results relating to the sociodemographic profile of the people affected by leprosy who took part in the study showed a higher frequency of males of brown color/race, illiterate, and with a family income of between R$1.200,00 and R$2.400,00 (Brazilian Reais) (Table 1).
When sociodemographic variables were assessed about impaired quality of life, the highest percentages of impairment were observed in male Black people, followed by Brown people, people with no schooling, and those with incomplete higher education, as well as those with a family income of between R$1.200,00 and R$2.400,00 (Brazilian Reals) (Table 1).
Table 1. Sociodemographic variables, according to impairment of the quality of life of people affected by leprosy treated at the Health Units of the Municipality of Pinheiro – MA. Pinheiro (MA), Brazil, 2023.
|
VARIABLES |
n.º |
% |
QUALITY OF LIFE SCORE |
|||||||
|
1 |
2 |
3 |
5 |
|||||||
|
n.º |
% |
n.º |
% |
n.º |
% |
n.º |
% |
|||
|
Gender |
||||||||||
|
Male |
13 |
72.22 |
3 |
23.08 |
5 |
38.46 |
4 |
30.77 |
1 |
7.69 |
|
Female |
5 |
27.78 |
2 |
40.00 |
2 |
40.00 |
1 |
20.00 |
0 |
00.00 |
|
Color/Race |
||||||||||
|
Brown |
12 |
66.67 |
3 |
25.00 |
6 |
50.00 |
2 |
16.67 |
1 |
8.33 |
|
Black |
5 |
27.78 |
1 |
20.00 |
1 |
20.00 |
3 |
60.00 |
0 |
0.00 |
|
White |
1 |
5.56 |
1 |
100.00 |
0 |
00.00 |
0 |
00.00 |
0 |
00.00 |
|
Education |
||||||||||
|
Illiterate |
5 |
27.78 |
0 |
0.00 |
2 |
40.00 |
3 |
60.00 |
0 |
00.00 |
|
Incomplete Elementary School |
3 |
16.67 |
1 |
33.33 |
0 |
00.00 |
1 |
33.33 |
1 |
33.33 |
|
Complete Elementary School |
2 |
11.11 |
1 |
50.00 |
1 |
50.00 |
0 |
00.00 |
0 |
00.00 |
|
Complete High School |
4 |
22.22 |
1 |
25.5 |
2 |
50.00 |
1 |
25.5 |
0 |
00.00 |
|
Incomplete Higher Education |
1 |
5.56 |
0 |
00.00 |
1 |
100.00 |
0 |
00.00 |
0 |
00.00 |
|
Complete Higher Education |
3 |
16.67 |
2 |
66.67 |
1 |
33.33 |
0 |
00.00 |
0 |
00.00 |
|
Family income (in Brazilian Reais) |
||||||||||
|
< 1.200,00 |
4 |
22.22 |
1 |
25.00 |
2 |
50.00 |
0 |
00.00 |
1 |
25.00 |
|
1.200,00 - 2.400,00 |
10 |
55.56 |
2 |
20.00 |
3 |
30.00 |
5 |
50.00 |
0 |
00.00 |
|
> 2.400,00 |
4 |
22.22 |
2 |
50.00 |
2 |
50.00 |
0 |
00.00 |
0 |
00.00 |
|
Total |
18 |
100.0 |
5 |
27.78 |
7 |
38.89 |
5 |
27.78 |
1 |
5.56 |
Key: 1 = No commitment; 2 = Mild commitment; 3 = Moderate commitment; 5 = Severe commitment.
As for clinical characteristics, the multibacillary operational classification of the disease predominated. The highest percentage was zero regarding the degree of physical disability at diagnosis. The highest percentage was zero regarding the family history of leprosy. When analyzing the duration of the disease, the highest frequency was among those who reported less than one year (Table 2).
In terms of clinical variables, impairment was more common among those with the multibacillary operational classification, who had grade II physical disability, who reported a history of leprosy in the family, and a disease duration of less than a year (Table 2).
Table 2. Clinical variables, according to impairment of quality of life of people affected by leprosy treated at Health Units in the Municipality of Pinheiro – MA. Pinheiro (MA), Brazil, 2023.
|
VARIABLES |
nº |
% |
QUALITY OF LIFE SCORE |
|||||||
|
1 |
2 |
3 |
5 |
|||||||
|
nº |
% |
nº |
% |
nº |
% |
nº |
% |
|||
|
Operational classification |
||||||||||
|
Paucibacillary |
7 |
38.89 |
3 |
42.86 |
4 |
57.14 |
0 |
00.00 |
0 |
00.00 |
|
Multibacillary |
11 |
61.11 |
2 |
18.18 |
3 |
27.27 |
5 |
45.45 |
1 |
9.09 |
|
Degree of physical disability |
||||||||||
|
0 |
8 |
44.44 |
4 |
50.00 |
3 |
37.50 |
1 |
12.50 |
0 |
00.00 |
|
1 |
6 |
33.33 |
1 |
16.67 |
3 |
50.00 |
2 |
33.33 |
0 |
00.00 |
|
2 |
4 |
22.22 |
0 |
00.00 |
1 |
25.00 |
2 |
40.00 |
1 |
25.00 |
|
Family history of leprosy |
||||||||||
|
Yes |
5 |
27.78 |
1 |
20.00 |
2 |
40.00 |
2 |
40.00 |
0 |
0.00 |
|
No |
13 |
72.22 |
4 |
30.77 |
5 |
38.46 |
3 |
23.08 |
1 |
7.69 |
|
Length of illness (years) |
||||||||||
|
< 1 year |
8 |
44.44 |
1 |
12.50 |
6 |
75.00 |
1 |
12.50 |
0 |
0.00 |
|
1 to 2 years |
6 |
33.33 |
3 |
50.00 |
0 |
0.00 |
2 |
33.33 |
1 |
16.67 |
|
> 2 years |
4 |
22.22 |
1 |
25.00 |
1 |
25.00 |
2 |
50.00 |
0 |
0.00 |
|
Total |
18 |
100.0 |
5 |
27.78 |
7 |
38.89 |
5 |
27.78 |
1 |
5.56 |
Key: 1 = No commitment; 2 = Mild commitment; 3 = Moderate commitment; 5 = Severe commitment.
In relation to the DLQI-BRA scores and the effect of leprosy on the patient's life, the following were identified: small effect, moderate effect, no effect and very large effect (Figure 1).
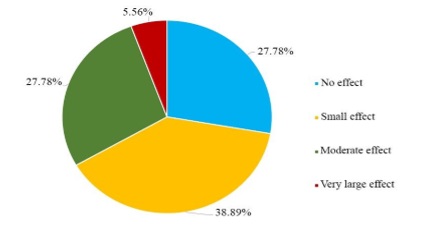
Figure 1. DLQI score of people affected by leprosy treated at health centers in Pinheiro – MA. Pinheiro (MA), Brazil, 2023.
In the analysis of quality of life, according to the questions/domains, it was found that all the domains were affected, with those relating to the questions “skin itchy, sensitive, sore or burning,” “shame or concern about appearance,” “choice of clothes” and “problems at work/school” being the most affected (Figure 2).
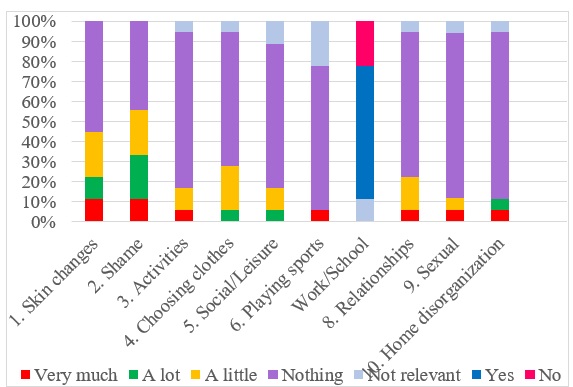 Figure 2. Quality of life of people affected by leprosy, according to questions/domains, municipality of Pinheiro – MA. Pinheiro (MA), Brazil, 2023.
Figure 2. Quality of life of people affected by leprosy, according to questions/domains, municipality of Pinheiro – MA. Pinheiro (MA), Brazil, 2023.
DISCUSSION
Leprosy is an infectious and transmissible disease that is chronic and persists as a public health problem10. It is distributed geographically, considering the spatial groupings identified as areas with an increased risk of disease cases, and, in Brazil, it does not present uniform characteristics. In Maranhão, most municipalities are part of areas with an elevated risk of leprosy22.
In the analysis of leprosy cases diagnosed in the municipality of Pinheiro-MA, males dominated, a finding repeated in most of the literature studied10,22. Some factors may be related to this predominance, such as more excellent social contact between men, exposure to risky environments, and fewer public policies and programs aimed at men's health, reducing the opportunity for early diagnosis23.
Regarding color/race, the higher frequency of cases in brown people was like national data for 2015 to 2019 and 202124,10.
Regarding the level of education, 27.78% of the patients were illiterate, showing that low levels of education are expected in epidemiological studies involving leprosy cases10,23. The illiteracy identified in this study was higher than that reported for new leprosy cases in the northeast and the state of Maranhão, which were 10.6% and 13.3%, respectively10. This shows that low levels of schooling continue to be directly linked to leprosy and can interfere with knowledge about the disease, making it difficult to detect, prevent, and understand guidelines on treatment and the necessary care23.
Cohort studies conducted in Brazil and India have also shown risk factors associated with becoming ill with leprosy related to illiteracy25. The family income of the people who took part in the study was around R$1.200,00 to 2.400,00 per month. As observed in Pinheiro, other authors have established that leprosy is associated with unfavorable socioeconomic conditions24.
Social vulnerability is an essential factor in the transmission of leprosy since socio-economic problems are directly related to malnutrition, inaccessibility to public services, high population density, and precarious housing conditions influencing the person's exposure and response to the disease agent26.
In scientific circles, in recent decades, research into discussions that emphasize the influence of social, economic, and cultural conditions on the population's morbidity and mortality profile has gained ground27. For this reason, local-regional research is necessary to find and identify priority areas for intervention, especially in regions with high endemicity parameters22.
The higher number of cases diagnosed as multibacillary is like that shown in numerous studies, representing late diagnosis and maintenance of the chain of transmission that contributes to the spread of the disease in the population22. In Brazil, there has been an increase in the proportion of new multibacillary cases, with an increase in all regions, with the highest proportion in the North and Northeast10.
As for the degree of physical disability assessed at the time of diagnosis, there was a higher frequency of cases with no physical disability (degree zero), also found in other studies10,22,28. People with physical disability in grades I and II, showing visible deformities because of the disease and reflecting late diagnosis, were also part of the study.
Early diagnosis is still the most crucial tool for timely treatment, breaking the chain of transmission of M. leprae and preventing the development of physical disabilities. Most cases of leprosy can be diagnosed in primary health care through clinical diagnosis19.
From 2012 to 2021, Brazil used a “regular” parameter to assess the degree of physical disability at the moment of diagnosis10.
When analyzing the history of leprosy cases in the family, the majority answered no, which agrees with reports in the current literature26. However, guidelines on assessing the contacts of an index case are essential. The literature describes that household contacts of people with multibacillary leprosy are up to eight times more likely to become ill28.
The period between the perception of signs and symptoms and the moment of diagnosis was less than a year. Similar data was found in a study on the sociodemographic, clinical, and geospatial profile of new leprosy cases diagnosed at the Lauro de Souza Lima Institute, Bauru, São Paulo, between 2015 and 2019. The time taken to diagnose the disease, after the first signs and symptoms, was less than a year in most cases26. However, in Pinheiro, cases with a delay of more than 24 months to diagnosis were also recorded. It is, therefore, necessary to understand what factors may be related to the delay in diagnosis, check whether users have barriers to accessing health services also and whether health professionals are having difficulties in the clinical management of leprosy patients after the COVID-19 pandemic in addition to observing whether the number of health services in the municipality is sufficient to provide care.
This scenario is worrying and may contribute to the perpetuation of the disease, raising serious concerns about the possibility of a hidden endemic26.
The DLQI-BRA was used to assess the quality of life among leprosy cases in the Pinheiro Health Units. When analyzing the sociodemographic and clinical data, relating them to the impairment of quality of life among people affected by the disease, it was found that males were predominant, as well as Black and Brown skin color/race among individuals who reported problems due to leprosy. Regarding the educational level of those interviewed, the study found high percentages of illiterate people with some impairment in their quality of life, which aligns with other literature. The population's low level of education can be a factor in the spread of the disease, as leprosy affects disadvantaged populations with a low level of knowledge, making control and prevention actions difficult24. Among the samples, one person had incomplete higher education and had an altered quality of life because of leprosy. This finding is rare and needs to be identified in the literature studied26.
The economic impact on the lives of people with leprosy directly affects their quality of life; most of the time, they have precarious living conditions, nutrition, hygiene, mobility, and difficulties in accessing health services. Multibacillary cases showed the most significant impairment of quality of life, corroborating data described by other authors24. Similarly, patients with physical disability grades I and II showed impairments that interfere with their quality of life, demonstrating the importance of early diagnosis and treatment of this disease to avoid sequelae29. In this study, people with a family history of leprosy and those who reported having been ill for less than a year had problems that interfered with their daily lives and, consequently, their quality of life.
In the DLQI-BRA, only 27.78% had no impairment in quality of life. The results are compatible with the literature, showing how much the disease affects people's lives. This reality may be due to the impact of leprosy on daily activities, interfering in the interaction of these individuals with the environment in which they are inserted in society24.
Regarding the evaluation of the DLQI questions/domains, based on the answers to the events that took place in the last week of the lives of people affected by leprosy (skin changes, shame, activities, choice of clothes, social life/leisure, playing sports, work/school, relationships, sex life, disorganization of the house), the results indicated that all the domains were affected, directly interfering with the quality of life.
The DLQI-BRA tool is valuable in quantifying subjective data, enabling evaluation beyond the clinical realm. Its role is pivotal in overcoming stigma and formulating a humanized proposal to enhance the quality of life of individuals affected by leprosy29.
In this context, nursing plays a vital role in the line of care and, together with the multi-professional team, contributes significantly to reducing leprosy's physical and psychosocial impact, improving care, reducing stigma and quality of life. However, the topic of leprosy must also be worked on in an intersectoral way involving other layers of society.
The limitations of this study include the COVID-19 pandemic and the related problems after the pandemic period that continue to challenge the single health system, whether in terms of its ability to maintain the supply of services, guarantee the necessary care for the target population, or maintain strategies to strengthen leprosy prevention and control actions, especially regarding surveillance, diagnosis, monitoring, and treatment of cases.
CONCLUSION
Analyzing the sociodemographic, clinical, and quality of life conditions of people affected by leprosy in this study can help improve actions to promote, prevent, and treat the disease.
In Brazil, leprosy is still considered a public health problem. Maranhão is a state with a highly high endemicity parameter for leprosy, as is the case in the municipality of Pinheiro-MA, and there is a need to improve epidemiological surveillance actions in line with the National Strategy to Combat Leprosy 2023-2030.
The study's evidence shows that tackling leprosy involves identifying vulnerable groups and requires intersectoral coordination to guarantee access to public policies such as social inclusion, education, income, and health services and strengthen leprosy control actions.
Actions should consider the profile of people with leprosy, especially men who do not attend health facilities and need to be encouraged to participate in public policies aimed at them; promote guidance on care through health education to reach those with little or no schooling; prevent physical disabilities, through active search, early diagnosis, and timely treatment; improve the offer of bacilloscopy in health services; expand access to services in the public health network; perform qualified listening and humanized care.
The academic community and researchers' interest in issues involving neglected diseases, such as leprosy, needs more encouragement from the federal units. Financial resources should be applied to scientific studies. Actions should focus on health care and management, prioritizing the Family Health Strategy.
CONTRIBUTIONS
Cristina Rosângela do Nascimento Carneiro: data collection, analysis, and interpretation; writing/critical review of the manuscript. Dorlene Maria Cardoso de Aquino: conception and planning of the study, data collection, analysis, and understanding. Estela Maria Leite Meirelles Monteiro: writing / critical revision of the manuscript. Ivan Abreu Figueiredo: writing / critical revision of the manuscript. Nair Portela Silva Coutinho: drafting /critical revision of the manuscript.
CONFLICT OF INTEREST
Nothing to declare.
FINANCING
This research comes from a UFMA project entitled “Clinical, Sociodemographic, Epidemiological and Operational Aspects of Leprosy in a Hyperendemic Municipality in the Baixada Maranhense”, funded by the Maranhão Foundation for Research Support and Scientific and Technological Development (FAPEMA), Universal Process-01135/19.
This study was supported by the Coordination for the Improvement of Higher Education Personnel (CAPES) under Funding Code 001, linked to the Postgraduate Program in Family Health PPGSF/RENASF/UFMA.
REFERENCES
- Ministério da Saúde. Guia de vigilância em saúde. 3. ed. Brasília: Ministério da Saúde; 2019. 740 p. [cited 28 fev 2023]. Available from: https://bvsms.saude.gov.br/bvs/publicacoes/guia_vigilancia_saude_3ed.pdf
- Dolenz MFA, Silva NMMG, Melo SCCS, Tashima CM, Toledo Neto JL, Bellucci Júnior JA, et al. Avaliação da qualidade de vida dos pacientes durante o tratamento e Hanseníase. Rev Odontologia (ATO). 2014 [cited 2023 Mar 5];14(4):238-256. Available from: https://www.researchgate.net/profile/Natalia-Guerra-Silva/publication/281108669_AVALIACAO_DA_QUALIDADE_DE_VIDA_DOS_PACIENTES_DURANTE_O_TRATAMENTO_DE_HANSENIASE/links/55d5e35f08aed6a199a2c7da/AVALIACAO-DA-QUALIDADE-DE-VIDA-DOS-PACIENTES-DURANTE-O-TRATAMENTO-DE-HANSENIASE.pdf
- Gaudenci EM, Nardelli GG, Almeida Neto OP, Malaquias BSS, Carvalho BT, Pedrosa LAK. Qualidade de vida, sintomas depressivos e incapacidade física de pacientes com hanseníase. Hansen Int. 2015 [cited 2023 Mar 27];40(2):48-58. DOI: https://doi.org/10.47878/hi.2015.v40.36175
- World Health Organization. Division of Health Promotion, Education and Communications (HPR); Health Education and Health Promotion Unit (HEP). Health Promotion Glossary. Genebra: WHO, 1998. 25p.
- Savassi LCM. Hanseníase: políticas públicas e qualidade de vida de pacientes e seus cuidadores [dissertação]. Belo Horizonte: Fundação Oswaldo Cruz; 2010 [cited 28 fev 2023]. Available from: https://www.cpqrr.fiocruz.br/texto-completo/D_48.pdf
- Minayo MCS, Hartz ZMA, Buss PM. Qualidade de vida e saúde: um debate necessário. Ciência & Saúde Coletiva. Rio de Janeiro, 2000;5(1):7-18. DOI: https://doi.org/10.1590/S1413-81232000000100002
- OMS (Organização Mundial da Saúde). Global leprosy (Hansen disease) update, 2021: moving towards interruption of transmission. Weekly Epidemiological Record, n. 36, p. 429-450, 9 set. 2022 [citado 10 jul. 2024]. Available from: https://www.who.int/ publications/i/item/who-wer9736-429-450
- Cavalcante MDMA, Larocca LM, Chaves MMN. Multiple dimensions of healthcare management of leprosy and challenges to its elimination. Rev Esc Enferm USP. 2020 [cited 28 fev 2023];54:e03649. DOI: https://doi.org/10.1590/S1980-220X2019010703649
- Mendonça IMS, Eleres FB, Silva EMS, Ferreira SMB, Sousa GS. Impacto da pandemia de Covid-19 no atendimento ao paciente com hanseníase: estudo avaliativo sob a ótica do profissional de saúde. Res Soc Dev. 2022 [cited 2023 abr 19];11(2):e4111225459. DOI: https://doi.org/10.33448/rsd-v11i2.25459
- Ministério da Saúde (BR). Boletim Epidemiológico: Hanseníase - 2023. Número Especial. Brasília, DF; 2023 [citado 20 ago. 2023]. Available from: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/especiais/2023/boletim_hanseniase-2023_internet_completo.pdf
- Passos CEC, Silva AR, Gonçalves EGR, Neiva FGC, Monteiro SG. Hanseníase no Estado do Maranhão: análise das estratégias de controle e os impactos nos indicadores epidemiológicos. Hygeia. 2016 [cited 2023 abr 19];12(22):88-100. DOI: https://doi.org/10.14393/Hygeia1230888
- Torres DC, Pinho KS, Borges CKS, Lopes AB, Costa GP, Gonçalves MC, et al. Comparação da qualidade de vida de indivíduos com e sem hanseníase. Rev Ceuma Perspectivas. 2019 [cited 2023 abr 25];30(2):64-77. DOI: https://doi.org/10.24863/rccp.v30i2.152
- Sistema de Informação de Agravo de Notificação (SINAN). Portal do Governo Brasileiro. Maranhão. 2021 [cited 25 mai 2022]. Available from: https://portalsinan.saude.gov.br/
- OMS (Organização Mundial da Saúde). Estratégia Global de Hanseníase 2021-2030 “Rumo à zero hanseníase”. Nova Deli: OMS, 2021 [cited 17 abr 2022]. Available from: https://www.who.int/pt/publications/i/item/9789290228509
- World Health Organization. Estratégia Global para Hanseníase 2016-2020: aceleração rumo a um mundo sem hanseníase. Nova Deli: WHO; 2017 [cited 28 mai 2022]. Available from: https://iris.who.int/bitstream/handle/10665/208824/9789290225201-pt.pdf
- Secretaria de Estado da Saúde (MA). Macrorregião de Saúde. Diário Oficial do Estado do Maranhão. 2018 [cited 20 fev. 2023]; (120):2-22. Available from: https://www.mpma.mp.br/arquivos/CAOPSAUDE/Anexo_Resolu%C3%A7%C3%A3o_CIBMA_n%C2%BA_64-2018.pdf
- Instituto Brasileiro de Geografia e Estatística (BR). Cidades e Estados - Pinheiro. 2021 [cited 20 fev 2023]. Available from: https://www.ibge.gov.br/cidades-e-estados/ma/pinheiro.html
- Cadastro Nacional de Estabelecimentos de Saúde (CNES). Portal do Governo Brasileiro. Pinheiro, MA; 2022 [cited 25 fev 2023]; Available from: https://cnes.datasus.gov.br/pages/estabelecimentos/consulta.jsp?search=PINHEIRO
- Ministério da Saúde (BR). Protocolo clínico e diretrizes terapêuticas da hanseníase. 1. ed. Brasília, DF; 2022 [cited 25 fev 2022]; Available from: https://bvsms.saude.gov.br/bvs/publicacoes/protocolo_clinico_diretrizes_terapeuticas_hanseniase.pdf
- Finlay AY and Khan GK. Dermatology Life Quality Index (DLQI): a simple practical measure for routine clinical use. Clin Exp Dermatol 1994; v.19, n.3: 210-216. [cited 25 maio 2023]. Available from: https://academic.oup.com/ced/article-abstract/19/3/210/6629483?redirectedFrom=fulltext#no-access-message
- Ministério da Saúde (BR). Secretaria de Atenção Primária à Saúde. Protocolo de Manejo Clínico do Coronavírus (Covid-19) na Atenção Primária à Saúde. Versão 9, Brasília, DF; maio de 2020 [cited 15 mar 2023]. Available from: https://www.unasus.gov.br/especial/covid19/pdf/37
- Rangel MES. Dinâmica espacial e contingências socioambientais da hanseníase no estado do Maranhão: avaliação de risco e vulnerabilidade em área hiperendêmicas [tese]. São Paulo: Universidade de São Paulo; 2016 [cited 2023 maio 23]. Available from: https://teses.usp.br/teses/disponiveis/8/8135/tde-02122016-122002/publico/2016_MauricioEduardoSalgadoRangel_VCorr.pdf
- Sá SC, Silva DS. Perfil epidemiológico da hanseníase em um município da região norte do Brasil. Braz J Dev. 2021 [cited 20 fev 2023];7(1):8959-8974. DOI: https://doi.org/10.34117/bjdv7n1-608
- Fortunato CN, Silva ACO, Mendes MS, Silva Júnior SV, Silva AB, Freire MEM. Qualidade de vida de pessoas com hanseníase atendidas em um hospital de referência, Paraíba-Brasil. Enferm Glob. 2019 [cited 20 fev 2023]; 56:133-145. DOI: http://dx.doi.org/10.6018/eglobal.18.4.342601
- Niitsuma ENA, Bueno IC, Arantes EO, Carvalho APM, Junior GFX, Fernandes GR, et al. Factors associated with the development of leprosy in contacts: a systematic review and meta-analysis. Rev Bras Epidemiol 2021[cited 11 jul 24]; 24: e 210039. DOI: https://doi.org/10.1590/1980-549720210039
- Chagas LBMO, Oliveira NG, Baptista IMFD, Souza VNB. Perfil sociodemográfico, clínico e geoespacial de casos novos de hanseníase diagnosticados no Instituto Lauro de Souza Lima, Bauru, São Paulo, entre 2015 e 2019. Hansen. Int. 2021 [cited 27 maio 23]; 46:1-22. DOI: https://doi.org/10.47878/hi.2021.v46.37428
- Barreto ML. Desigualdades em Saúde: uma perspectiva global. Ciênc Saúde Coletiva. 2017 [cited 20 nov. 2022];22(7):2097-2108. DOI: https://doi.org/10.1590/1413-81232017227.02742017
- Pedrosa VL, Dias LC, Galban E, Leturiondo A, Palheta Jr J, Santos M, et al. Leprosy among schoolchildren in the Amazon region: a cross-sectional study of active search and possible source of infection by contract tracing. PLoS Negl Trop Dis. 2018 [cited 27 maio 23];12(2):e0006261. DOI: https://doi.org/10.1371/journal.pntd.0006261
- Castro RNC, Veloso TC, Matos Filho LJS, Coelho LC, Pinto LB, Castro AMNC. Avaliação do grau de incapacidade física de pacientes com hanseníase submetidos ao Dermatology Quality Life Index em Centro de Referência e Unidades Básicas de Saúde de São Luis, MA. Rev Bras Clin Med. 2009 [cited 27 maio 23]; 7:390-392. Available from: http://files.bvs.br/upload/S/1679-1010/2009/v7n6/a007.pdf
Correspondence
Cristina Rosângela do Nascimento Carneiro
E-mail: cris_rosangel@hotmail.com
Copyright© 2024 Revista de Enfermagem UFPE on line/REUOL.
This open-access article is distributed under the CC BY 4.0 Creative Commons Attribution-ShareAlike 4.0 International License, allowing others to distribute, remix, adapt, and create from your work, even for commercial purposes, if they credit you for the original creation. Maximizing the dissemination and use of licensed materials is recommended.
 Português (Brasil)
Português (Brasil)  English
English  Español (España)
Español (España) 



















