
Idioma
Physical disabilities due to leprosy: sociodemographic and clinical profile in a brazilian Amazon state
INTRODUCTION
Caused by Mycobacterium leprae, leprosy is a chronic infectious disease with slow evolution. Although it is old and presents control strategies, it persists as a global public health concern, causing many socioeconomic, physical and psychological repercussions for those affected. Manifesting with dermatoneurological signs and symptoms, it affects people of both sexes and all age groups. When diagnosed and treated late, or if left untreated, it can develop physical disabilities (PD) in the hands, feet and/or face due to neural impairment.1
PD affect the quality of life and prevent or limit the execution of activities of daily living, contributing to social stigma caused by the disease, evidenced by conditions that increase vulnerability, such as unemployment, deterioration of psychosocial health and perpetuation of cycles of poverty and social exclusion. In view of this, neural function assessment is essential in diagnosis, during and after treatment, in the occurrence of neuritis and in reactional states, in order to assess grade of physical disability (GPD) and prevent complications.2-3
To reduce leprosy and PD detection rates, the World Health Organization (WHO) developed the Global Leprosy Strategy 2021-2030. This initiative aims at early detection and immediate treatment, searching for contacts of all new cases and diagnosing and treating leprosy reactions, neuritis and PD so that the effectiveness of actions to control the disease can be achieved in all territories, with their different endemicities.1
In Brazil, the distribution of the disease is heterogeneous and constitutes a problem related to socioeconomic inequality, regarding the level of education and precarious basic sanitation and housing conditions, making it possible to infer that the North and Northeast regions are the most affected by the spread of the disease.3 In 2021, the state of Pará ranked third with the highest leprosy detection rate in the North region, with 18.62 new cases per 100 thousand inhabitants, the first in the region in absolute numbers, with 1,634 cases. Regarding PD, in the same year, the rate of new cases with PD grade 2, in Pará, was 17.09 per one million inhabitants, corresponding to the third highest rate in the North region.4
Based on the need to know the epidemiological profile of leprosy, emphasizing PD that arise from it, this reality justifies the relevance of this study. Information about this profile is essential to provide support to managers and healthcare professionals, with the aim of planning health surveillance, disease prevention and control actions, through differentiated strategies, which meet the individual and collective needs of different territories, in accordance with the Global Strategy.5
OBJECTIVE
To describe the sociodemographic and clinical profile of leprosy cases with GPD assessed at the time of diagnosis.
METHOD
This is an epidemiological, descriptive and retrospective study, carried out with data from the Notifiable Diseases Information System (SINAN - Sistema de Informação de Agravos de Notificação), collected in September 2020 at the Pará Department of Public Health (SESPA - Secretaria de Estado de Saúde Pública do Pará). The recommendations of Strengthening the Reporting of OBservational studies in Epidemiology (STROBE),6 instrument of Enhancing the QUAlity and Transparency Of health Research (EQUATOR Network), were followed.
We included leprosy cases residing in the state of Pará, reported between 2009 and 2018, of both sexes, with GPD assessed at the time of diagnosis. We chose to exclude duplicate notifications, with incomplete information or inconsistencies in the SESPA database.
Initially, 20,096 cases were identified in the historical series. When refining the database, 610 were excluded, leaving 19,486, which presented information about the GPD assessed at the time of diagnosis, constituting the final sample.
PD (classified as grades 0, 1 and 2), sociodemographic (sex, age and education) and clinical (operational classification from the Ministry of Health, clinical form and number of affected nerves) variables were chosen. The variables were decoded, according to the SINAN Net data dictionary and the script for using SINAN Net in the context of leprosy.7-8 They were then tabulated in a Microsoft Office Excel® version 2016 spreadsheet.
Ignored, unclassified or unevaluated variables were excluded, enabling bivariate analysis. By using Microsoft Office Excel® 2016 and the International Business Machines Statistical Package for the Social Sciences (IBM SPSS) Statistics® version 23.0, parametric and non-parametric data were analyzed, respectively.
Using descriptive statistics, absolute and relative frequencies, mean and standard deviation for quantitative variables were calculated, and frequency distribution was also performed for qualitative variables. With inferential statistics, Pearson’s non-parametric chi-square test was applied to verify the dependence between variables. Statistical associations were identified from the contingency table, with a 5% significance level (p<0.05) and a 95% Confidence Interval.
To characterize the temporal evolution of leprosy cases, two epidemiological indicators were calculated, recommended by the Ministry of Health: 1) general detection rate of new cases (number of new cases residing in a given location and diagnosed in the year of assessment/total population resident, in the same location and year of assessment), which measures the strength of morbidity, magnitude and trend of the disease; 2) proportion of new cases with GPD 2 at the time of diagnosis (number of new cases with GPD 2, residing in a given location and detected in the year of assessment/total number of new cases with GPD assessed, residing in the same location and year of assessment), which measures the effectiveness of timely and/or early case detection activities.4
In the first indicator, five classification parameters were considered: low (<2.00 cases per 100 thousand inhabitants); medium (2.00 to 9.99 cases per 100 thousand inhabitants); high (10.00 to 19.99 cases per 100 thousand inhabitants); very high (20.00 to 39.99 cases per 100 thousand inhabitants); and hyperendemic (≥40.00 cases per 100 thousand inhabitants). In turn, in the second indicator, the parameters were: low (≤5.0%); medium (5.0% to 9.9%); and high (≥10.0%).4 The calculations for both were carried out considering the 2010 Demographic Census, made available in a virtual environment of the Brazilian Institute of Geography and Statistics (IBGE - Instituto Brasileiro de Geografia e Estatística), whose access is public.9
This study met the recommendations of Resolution 466/2012 of the Brazilian National Health Council, obtaining approval from the Universidade do Estado do Pará (UEPA) Undergraduate Nursing Course Research Ethics Committee, under Opinion 4.241.488.
RESULTS
Of the 19,486 cases of leprosy, it was identified that 4,806 (24.66%) had GPD 1, and 1,351 (6.93%), GPD 2, totaling 6,157 (31.60%) cases of PD. The statistically significant sociodemographic factors, when associated with cases with PD, were being male (n=4,213; 21.62%; p<0.0001), mean age of approximately 39 years, with a standard deviation of ±18, 48 (p<0.0001), and incomplete elementary school (n=3,607; 18.51%; p<0.0001), indicating a predominance of low education (Table 1).
Table 1. Distribution of leprosy cases, by grade of physical disability, according to sociodemographic variables, 2009 to 2018 (n=19,486). Belém (PA), Brazil, 2023.
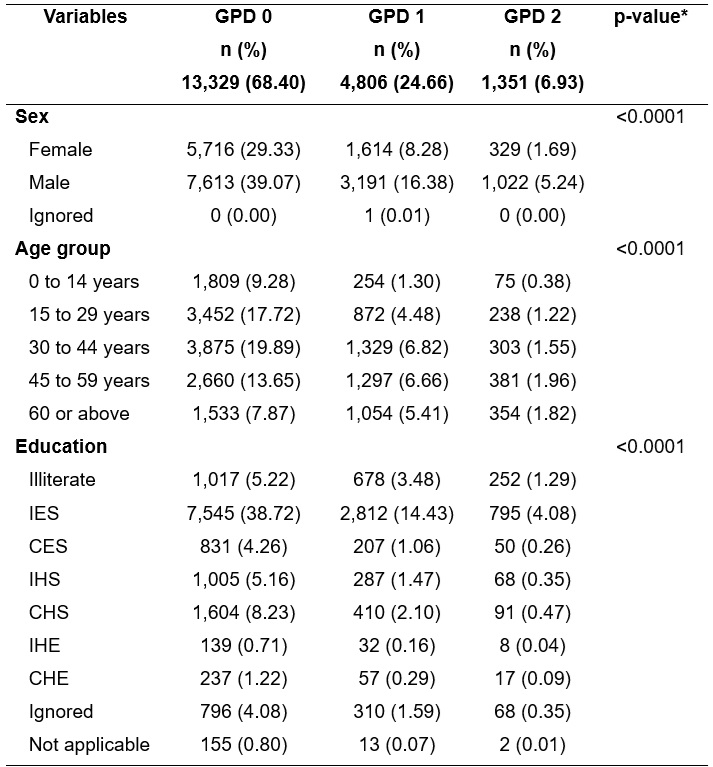
Note: GPD - grade of physical disability; IES - incomplete elementary school; CES - complete elementary school; IHS - incomplete high school; CHS - complete high school; IHE - incomplete higher education; CHE - complete higher education.
*Pearson’s chi-square test.
Source: SINAN/SESPA.
In Table 2, the statistical association of GPD 1 and 2 with clinical variables can be seen, with the predominance of multibacillary operational classification (n=5,665; 29.07%; p<0.0001) and dimorphic (n=3,887; 19.95%; p<0.0001) and Virchowian (n=1,447; 7.43%; p<0.0001) clinical forms. It is also noted that 5,313 (27.27%; p<0.0001) cases with GPD 1 and 2 had one or more affected nerves.
Table 2. Distribution of leprosy cases, by grade of physical disability, according to clinical variables, 2009 to 2018 (n=19,486). Belém (PA), Brazil, 2023.
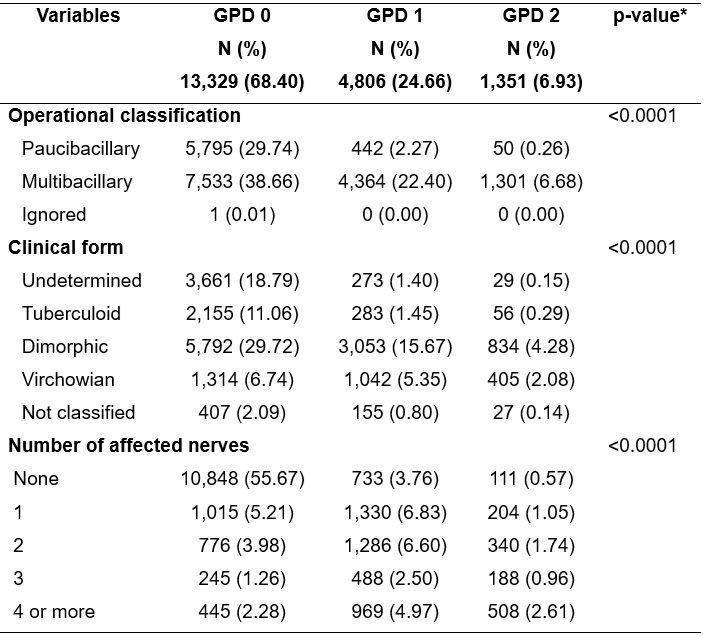
Note: GPD - grade of physical disability.
*Pearson’s chi-square test.
Source: SINAN/SESPA.
In the temporal evolution of cases, a very high parameter was identified, for all years, in relation to the general detection rates of new cases, and a mean parameter, in all years, in relation to the proportions of new cases with GPD 2. Furthermore, in the historical series, there was: upward trend in case detection rates between 2009 and 2012; downward trend of these rates from 2013 to 2018, with the exception of 2014 and 2017, in which small increases were recorded, followed by drops; and linear trend of PD proportions, with discrete variaions, as shown in Figure 1.
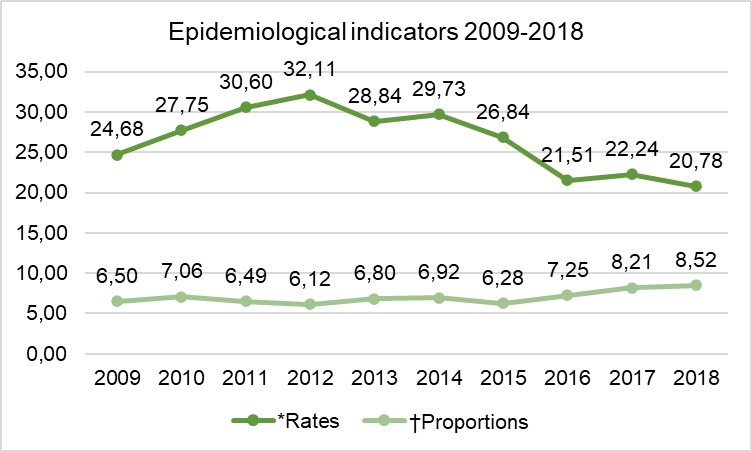
Figure 1. General detection rates of new leprosy cases and proportions of new cases with grade of physical disability 2, 2009 to 2018 (n=19.486). Belém (PA), Brazil, 2023.
Note: *General detection rates of new leprosy cases.4; †Proportions of new leprosy cases with grade of physical disability 2 at the time of diagnosis.4
Source: SINAN/SESPA.
DISCUSSION
It was evident that cases of leprosy with PD affected, above all, the male population, in the age groups of 30 to 44 and 45 to 59 years, with education inherent to incomplete elementary school, multibacillary operational classification, dimorphic and Virchowian clinical forms, affecting one to two nerves (among cases with GPD 1) and four or more nerves (among cases with GPD 2). Among the cases analyzed, 31.60% presented GPD 1 and 2 at the time of diagnosis, signaling that the diagnosis of the disease occurred significantly late and that there are probably undiagnosed cases in the social environment.
Thus, although leprosy affects both sexes, it is worth considering that, in the state of Pará, men are affected more frequently, in line with other research, which reveals a higher percentage of men affected.5,10-11 This scenario is related to the frequent exposure of men to risky environments, greater social contact and the fact that, culturally, men show less concern about their health and greater concern about work activities and family support when compared to women. As a result, there is less demand for health services among men, contributing to increasing or maintaining the number of cases of the disease and PD caused by it.5,12-13
In this context, there was a statistically significant relationship between PD and sex, showing that 21.62% of leprosy cases with GPD 1 and 2 occurred in males. The fact shows that, in addition to the disease affecting men more often, it disables them more frequently, as it is diagnosed late. This result is supported by a case-control study, demonstrating that men were approximately three times more likely to develop PD than women.14 Thus, the findings of GPD 1 and 2 demonstrate the inefficiency of public health services in early identification of cases and in meeting their individual and collective needs.14
The age groups from 30 to 44 and 45 to 59 years stood out, identifying a statistically significant relationship between PD and age, with 16.99% of people aged 30 to 59 years affected by GPD 1 or 2, i.e., adults of economically active age. This result is in line with other studies, characterizing leprosy as an entity that, although it affects all age groups, represents a greater risk to adults.12,14-15 This also highlights the chronic nature of the disease, which has repercussions on work activities and, consequently, on the national economy, with an overload on the social security system.
In relation to endemicity in Pará, it is noteworthy that the age group inherent to those under 15 years accounted for 10.96% of cases, considering the three GPD. The incidence of leprosy in this range constitutes an indicator of the prevalence of the disease in the general population, and its detection signals early exposure to Mycobacterium leprae and active transmission cycles.5,10,14 In this age group, in the national territory, the endemic is considered high, and Pará, in 2021, ranked second in number of cases among children under 15 years in the country, a reality that highlights negligence in disease control by Primary Health Care (PHC) services.4,14
Despite the higher prevalence in adults, it is appropriate to highlight the need to assess intra-household contacts or contacts that are part of patients’ family/social circle, given that, in endemic areas, such as Pará, the risk of a child becoming ill is greater due to prolonged contact with a family member who lives with leprosy. Therefore, it sometimes presents itself as a subclinical disease, diagnosed in individuals already in adulthood and, possibly, with PD resulting from sequels. PHC teams must carefully investigate these contacts and people with dermatoneurological symptoms, in order to reduce the number of late diagnoses and cases with PD.14-15
Low education predominated in this study, with 11,152 (57.23%) cases among people with incomplete elementary school, considering the three GPD, approaching the results of several studies.14,16-17 This characteristic is associated with little information about the disease and, consequently, the delay in seeking health services, culminating in late treatment. Furthermore, it is known that low education is an obstacle to effectively understanding educational measures to promote health and prevent illness and to adhere to self-care and treatment of clinically challenging diseases, such as leprosy. Therefore, when considering this variable as an indicator of living conditions in the context of leprosy, its characteristic of a neglected tropical disease is reinforced.14,16-17
There was, therefore, a relationship between PD and education, a context in which 3,607 (18.51%) cases with incomplete elementary school presented PD 1 or 2, revealing the statistically significant dependence between these variables. This finding is in line with the literature, which points to low education as a risk factor for PD, since an increase in the level of education influences early diagnosis and, conversely, people with no education or only with elementary school have higher chances of being diagnosed with PD when compared to those with high school or higher education levels.17
Therefore, when contacting the community, it is important that PHC professionals provide information and raise awareness among the population about the early detection of the disease, encouraging, above all, men to attend health units to be regularly assessed. These activities can contribute to mitigating the difference in access to diagnosis and treatment as well as reducing the stigma of the disease, which inhibits the demand for health services due to fear of social isolation.17
As for clinical aspects, the majority of notifications were classified as multibacillary cases (67.74%), similar to several studies, which also demonstrated high percentages of this type of classification,11,18-19 in a context in which this number is close to the percentage national number of new multibacillary cases (80.2%), identified in 2022.4
This scenario reveals the seriousness of the situation in Pará, raising an alert to health authorities, due to the fact that multibacillary cases are responsible for maintaining the chain of transmission of the disease and for standing out as forms with significant disabling potential.2,19 Furthermore, contacts of people with the disease have up to ten times more risk of becoming ill from leprosy than the general population. To control the disease, it is essential, therefore, to assess contacts.14
When associating PD with operational classification, it was identified that 29.08% of PD cases were classified as multibacillary, showing statistical dependence between these variables. According to the Ministry of Health, the proportion of multibacillary cases is a risk indicator for developing leprosy complications and is related to the perpetuation of the transmission chain and the hidden prevalence of the disease.2
GPD is an epidemiological indicator that can be used to assess the leprosy surveillance program’s actions, determining early diagnosis and the success of transmission control activities, which is why the proportion of multibacillary cases is related to GPD. Therefore, to prevent complications such as PD and leprosy reactions, early diagnosis and neurological evaluation at the time of diagnosis are very important.2,4
In cases with GPD 1 and 2, dimorphic (19.95%) and Virchowian (7.43%) clinical forms predominated. Other studies reveal that multibacillary cases are at greater risk of developing neural involvement, an association that can lead to PD.14,18,20
Most (60.00%) cases occurred that did not present nerve involvement due to the disease. However, associating PD and number of affected nerves, it was identified that 4.33% of PD cases did not affect the nerve and 16.22% had one to two affected nerves. Similarly, a high prevalence of leprosy cases without nerve involvement was a finding of another study in Pará.18
Despite the high percentage of cases without nerve involvement, cases of leprosy in Pará are still, partially, detected late, with a greater probability of active transmission of the disease and neural complications. In view of this, the importance of training health professionals for adequate dermatoneurological assessment and early detection and treatment of the disease stands out, considering that people with affected nerves are more likely to experience sequels with some GPD.18,21
Thus, the lack or lack of professional qualifications stands out as another factor that leads to late diagnosis, a context in which patients often develop PD even before receiving the first specific care. Public health services still do not detect all those affected in a timely manner, contributing to maintaining the transmission chain and the development of PD, with consequent limitations in social life, which generate psychological problems and reduced quality of life. Therefore, it is necessary to qualify continuing education processes, especially for PHC professionals, in order to strengthen knowledge, attitudes and skills, increasing suspicion of the disease to avoid transmission and possible complications.21
Concerning the temporal behavior of the general detection rates of new cases, the perpetuation of the very high parameter was evident throughout the entire historical series, with a downward trend in the last six years, 2013 to 2018, with the exception of 2014 and 2017, which showed a slight increase in relation to the years that preceded them. Rate regression results were found in other research on the temporal evolution of leprosy in Sobral, state of Ceará,10 and in municipalities in the state of Minas Gerais.22 Even with a reduction in rates, the values shown in Pará are higher than those reported verified in other realities in the national territory.4
The trends shown by epidemiological indicators over a given period have been widely used as they are more enlightening and reliable than the information obtained through analyzes of isolated cases.20-22 In this regard, the case detection rate is one of the most useful indicators to assess the magnitude of leprosy in a given area, reflecting not only the epidemiological characteristics of the disease, but also operational problems in the organization of services to control it.10
Regarding the proportion of new cases with GPD 2 assessed at the time of diagnosis, a linear trend in the proportions of PD was observed, with variation between the minimum proportion of 6.12%, in 2012, and the maximum of 8.52%, in 2018, however, all within the mean parameter. Investigating this indicator allows assessing the effectiveness of early case detection actions, showing the effectiveness of disease control programs.10 Therefore, even if the parameter identified in this study is average, any proportion of cases with PD is important, as it demonstrates late diagnosis and hidden prevalence, maintaining the transmission chain.22
Thus, PD rates may be associated with the low effectiveness of detection actions and difficulties in accessing health services in Pará, revealing that these services present difficulties in carrying out control activities, as recommended by the Ministry of Health.21 It is noteworthy that GPD assessment is essential for planning health actions, with the aim of preventing the progression of the disease, disabilities and physical deformities. The earlier leprosy is diagnosed, the GPD tends to be lower; however, complications are still a challenge for services, as the onset of the disease occurs insidiously, without symptoms and, in many cases, this can explain the delay in diagnosis as a risk factor for PD.2,21-22
When considering the particular bias of using secondary data, this study presents, as a limitation, duplications, incompleteness and/or inconsistencies in excluded data. This occurs due to possible failures in case investigation/notification processes and/or data entry into the information system. However, the data were treated with methodological rigor and are representative to demonstrate the epidemiological situation of leprosy in Pará during the period studied.
CONCLUSION
The state of Pará showed high endemicity, active transmission and late diagnosis of leprosy, with a very high parameter of general detection rates of new cases and mean proportions of GPD 2 in the period studied. This reality increases the recognition of the disease as a public health concern, especially in the local-regional context, intertwining with morbidity, recent and persistent transmission of the disease, late diagnosis and the probable endemic hidden by the high numbers of multibacillary cases and cases of PD.
In addition to epidemiological control and surveillance actions, recommended by the Ministry of Health, the importance of active search strategies, in accordance with the territorial reality, and health education actions carried out with human groups, aiming at early diagnosis and treatment, stands out. In this way, when showing signs and symptoms, and suspecting the disease, people will be able to seek health services in a timely manner to be assessed.
It is also reiterated the need to encourage spaces for continuing education among health professionals to better train them and to develop care processes based on technical-scientific knowledge, good practices and ethical-humanistic precepts, strengthening health care actions control.
It is hoped that the results of this study will reach professionals, especially in PHC, so that they can reflect and pay attention to the importance of activities to prevent PD, search for contacts, dermatoneurological assessment, guidance on self-care practices and, above all, the consequences of late diagnosis, which causes patients to develop irreversible PD. It is understood, therefore, that the results presented here may support other studies to expand the fight against the disease in the fields of health care, management, teaching and research.
CONTRIBUTIONS
Soares AS, Duarte BAS, Oliveira LF and Almeida MGC: study design, collection, data analysis and interpretation, writing and critical review of the manuscript. Andrade EGR and Borges MO: data analysis and interpretation, writing and critical review of the manuscript. Rodrigues ILA, Nogueira LMV: writing and critical review of the manuscript.
CONFLICT OF INTERESTS
Nothing to declare.
FINANCING
UEPA – Granting of a scholarship to the first author, through the Institutional Scientific Initiation Scholarship Program (PIBIC - Programa Institucional de Bolsas de Iniciação Científica) – UEPA Notice 013/2019. Grant code: 31403. Proc: 19/88824.
REFERENCES
- World Health Organization, Regional Office for South-East Asia. Global Leprosy (Hansen’s disease) Strategy 2021-2030: Towards Zero Leprosy [Internet]. Nova Delhi (IN): World Health Organization; 2021 [cited 2022 June 16]. 29 p. Available from: https://www.who.int/publications/i/item/9789290228509
- Ministério da Saúde (BR), Secretaria de Vigilância em Saúde, Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis. Protocolo clínico e diretrizes terapêuticas da hanseníase [Internet]. Brasília (DF): Ministério da Saúde; 2022 [cited 2024 Feb 02]. 152 p. Available from: https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/h/hanseniase/publicacoes/protocolo-clinico-e-diretrizes-terapeuticas-da-hanseniase-2022
- Pescarini JM, Teixeira CSS, Silva NB, Sanchez MN, Natividade MS, Rodrigues LC, et al. Epidemiological characteristics and temporal trends of new leprosy cases in Brazil: 2006 to 2017. Cad Saúde Pública. 2021;37(7):e00130020. DOI: https://doi.org/10.1590/0102-311X00130020
- Ministério da Saúde (BR), Secretaria de Vigilância em Saúde, Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis. Boletim epidemiológico de hanseníase 2023 [Internet]. Brasília (DF): Ministério da Saúde; 2023 Jan [cited 2023 May 28]. 51 p. Available from: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/especiais/2023/boletim_hanseniase-2023_internet_completo.pdf/view
- Tavares AMR. Epidemiological profile of leprosy in the state of Mato Grosso: descriptive study. Einstein (São Paulo). 2021;19:eAO5622. DOI: https://doi.org/10.31744/einstein_journal/2021AO5622
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10):e296. DOI: https://doi.org/10.1371/journal.pmed.0040296
- Ministério da Saúde (BR), Secretaria de Vigilância em Saúde, Departamento de Vigilância Epidemiológica, Centro de Informações Estratégicas em Vigilância em Saúde, GT-SINAN. Sistema de Informação de Agravos de Notificação: dicionário de dados – SINAN Net – versão 5.0 [Internet]. Brasília (DF): Ministério da Saúde; 2020 [cited 2020 Jan 06]. 8 p. Available from: http://portalsinan.saude.gov.br/images/documentos/Agravos/Hanseniase/DIC_DADOS_Hanseniase_v5.pdf
- Ministério da Saúde (BR), Secretaria de Vigilância em Saúde, Departamento de Vigilância Epidemiológica das Doenças Transmissíveis, Coordenação Geral de Hanseníase e Doenças em Eliminação, Unidade Técnica do SINAN. Roteiro para uso do Sistema de Informação de Agravos de Notificação – SINAN Net para hanseníase – Manual para tabulação dos indicadores de hanseníase: versão preliminar [Internet]. Brasília (DF): Ministério da Saúde; 2019 [cited 2020 Jan 06]. 100 p. Available from: http://portalsinan.saude.gov.br/images/documentos/Agravos/Hanseniase/Manual_indicadores_hanseniase.pdf
- Instituto Brasileiro de Geografia e Estatística. Base de dados – Censo 2010: estado do Pará [Internet]. Rio de Janeiro (RJ): IBGE; 2020 [cited 2020 Jan 06]. Available from: https://cidades.ibge.gov.br/brasil/pa/panorama
- Pereira TM, Silva LMS, Dias MSA, Monteiro LD, Silva MRF, Alencar OM. Temporal trend of leprosy in a region of high endemicity in the Brazilian Northeast. Rev Bras Enferm. 2019;72(5):1356-62. DOI: https://doi.org/10.1590/0034-7167-2018-0682
- Cisneros J, Ferreira JA, Grossi MAF, Filippis T, Oliveira ALG, Lyon S, et al. Associations between occupation, leprosy disability and other sociodemographic factors in an endemic area of Brazil. PLoS Glob Public Health. 2022;2(9):e0000276. DOI: https://doi.org/10.1371/journal.pgph.0000276
- Alves JM, Rodrigues RP, Carvalho MCS. Epidemiological and spatial profile of new leprosy cases notified at Feira de Santana (Brazil) between 2005 and 2015. Rev Pesqui Fisioter. 2021;11(2):334-41. DOI: http://dx.doi.org/10.17267/2238-2704rpf.v11i2.3682
- Beia T, Kielmann K, Diaconu K. Changing men or changing health systems? A scoping review of interventions, services and programmes targeting men’s health in sub-Saharan Africa. Int J Equity Health. 2021;20:87. DOI: https://doi.org/10.1186/s12939-021-01428-z
- Véras GCB, Lima Júnior JF, Cândido EL, Maia ER. Risk factors for physical disability due to leprosy: a case-control study. Cad Saúde Colet. 2021;29(3):411-23. DOI: https://doi.org/10.1590/1414-462X202129030182
- Coriolano CRF, Freitas Neto WA, Penna GO, Sanchez MN. Fatores associados ao tempo de ocorrência das reações hansênicas numa coorte de 2008 a 2016 em Rondônia, Região Amazônica, Brasil. Cad Saúde Pública. 2021;37(12):e00045321. DOI: https://doi.org/10.1590/0102-311X00045321
- Boigny RN, Souza EM, Romanholo HSB, Araújo OD, Araújo TME, Carneiro MAG, et al. Persistência da hanseníase em redes de convívio domiciliar: sobreposição de casos e vulnerabilidade em regiões endêmicas no Brasil. Cad Saúde Pública. 2019;35(2):e00105318. DOI: https://doi.org/10.1590/0102-311X00105318
- Lopes FC, Ramos ACV, Pascoal LM, Santos FS, Rolim ILTP, Serra MAAO, et al. Leprosy in the context of the Family Health Strategy in an endemic scenario in Maranhão: prevalence and associated factors. Ciênc Saúde Colet. 2021;26(5):1805-16. DOI: https://doi.org/10.1590/1413-81232021265.04032021
- Silva JSR, Palmeira IP, Sá AMM, Nogueira LMV, Ferreira AMR. Variáveis clínicas associadas ao grau de incapacidade física na hanseníase. Rev Cuid. 2019;10(1):e618. DOI: http://dx.doi.org/10.15649/cuidarte.v10i1.618
- Oliveira KS, Arcoverde MAM, Deschutter EJ, Silva AJ, Zilly A, Sobrinho RAS. Leprosy in border countries in South America: an ecological study. Cogitare Enferm. 2019;24:e64917. DOI: http://dx.doi.org/10.5380/ce.v24i0.64917
- Moreira RJO, Bezerra JM, Santos FS, Pascoal LM, Santos LH, Santos Neto M. Clinical-epidemiological characteristics and temporal trend of new cases of grade 2 disability leprosy in the state of Maranhão, Brazil, 2011- 2020. Epidemiol Serv Saúde [Internet]. 2023;32(2):e2022435. DOI: https://doi.org/10.1590/S2237-96222023000200026
- Damasceno PR, Gomes VAS, Souza AJS, Silveira MC, Laet AL, Santos GNV. Perfil clínico-epidemiológico de pessoas com hanseníase no estado do Pará entre os anos de 2017-2021. Rev Enferm Contemp. 2023;12:e4905. DOI: http://dx.doi.org/10.17267/2317- 3378rec.2023.e4905
- Bueno IC, Lages DS, Lana FCF. Spatial analysis of the epidemiological risk of leprosy in the municipalities of Minas Gerais. PLOS Neglected Tropical Diseases. 2023;17(6):e0011381. DOI: https://doi.org/10.1371/journal.pntd.0011381
Correspondence
Aloma Sena Soares
E-mail: alomassoares@gmail.com
Copyright© 2024 Revista de Enfermagem UFPE on line/REUOL.
Este é um artigo de acesso aberto distribuído sob a Atribuição CC BY 4.0 Creative Commons Attribution-ShareAlike 4.0 International License, a qual permite que outros distribuam, remixem, adaptem e criem a partir do seu trabalho, mesmo para fins comerciais, desde que lhe atribuam o devido crédito pela criação original. É recomendada para maximizar a disseminação e uso dos materiais licenciados.
 Português (Brasil)
Português (Brasil)  English
English  Español (España)
Español (España) 



















