
Idioma
Clinical and epidemiological profile of cancer patients undergoing outpatient chemotherapy
Pessanha RM1, D’Agostini NS2, Giacomin LM3, Busatto LS4, Amaral MC5, Souza ACSV6, Grippa WR7, Lopes-Júnior LC8.
1,2,3,4,5,6,7,8 - Federal University of Espírito Santo/UFES. Vitória (ES), Brasil.
INTRODUCTION
Cancer is one of the greatest challenges to global public health, with significant psychosocial and economic impacts. It stands as one of the leading causes of death worldwide.1 In this context, global epidemiological and demographic shifts directly influence cancer incidence and mortality.2,3 Factors such as population aging, environmental changes, and new lifestyle habits affect both the occurrence and outcomes of neoplasms.1,3
According to the most recent global estimates from GLOBOCAN 2022, approximately 19.9 million new cancer cases and 9.7 million cancer-related deaths were projected for the year 2022.4 In Brazil, the National Cancer Institute (INCA) estimates for the 2023–2025 period anticipate over 704,000 new cancer cases. Among the most frequent neoplasms are malignant breast, prostate, colon, and rectal cancers, which together account for over 190,000 new diagnoses.1,5 In Espírito Santo, the state where this study was conducted, the 2023 estimate was approximately 8,000 new cancer cases, excluding non-melanoma skin cancers. Of these, 3,360 cases were breast cancer, making it the second most prevalent type in the state.5
Chemotherapy is one of the most used treatments for cancer patients. Various chemotherapeutic agents are often combined to enhance outcomes at different stages of the disease. Chemotherapy can be classified as neoadjuvant, adjuvant, or palliative.6 According to 2020 DATASUS data, more than 2.5 million chemotherapy sessions are performed annually, accounting for over 48% of total cancer therapy expenditures within Brazil’s Unified Health System (SUS).7 Established in 1988 and regulated in 1990, the SUS provides universal and comprehensive health care services to the Brazilian population, aiming to reduce inequalities, particularly socioeconomic barriers that hinder access to health care.8 In this context, healthcare services and resources allocated to cancer treatment have a direct impact on mortality and survival rates in Brazil. Regions with low-income populations and less development tend to exhibit higher cancer mortality rates.6,9
Mapping the clinical and epidemiological profile of cancer patients undergoing treatment in the state of Espírito Santo aims to address a gap in the literature regarding the clinical, social, economic, and risk factors of oncology patients receiving outpatient chemotherapy. This descriptive study has the potential to shed light on these gaps and generate hypotheses for testing in analytical studies. Additionally, it can contribute to the development of public policies tailored to specific contexts and timely needs, thereby strengthening preventive and therapeutic strategies.
OBJECTIVE
This study aims to describe the clinical and epidemiological profile of cancer patients referred for outpatient chemotherapy.
METHOD
This is a descriptive observational study conducted at Afecc-Hospital Santa Rita de Cássia, the only High-Complexity Oncology Center (CACON) in the state of Espírito Santo (ES) and a reference institution for cancer treatment in the region.
The study included patients aged over 18 years, newly diagnosed with histopathologically confirmed malignant neoplasms in stages I, II, or III, and referred for outpatient chemotherapy. Excluded were patients in stage IV, those with more than one primary tumor, or those receiving exclusively palliative care.
The exclusion of these groups is justified by the fact that this study is part of a broader project that will evaluate, as a secondary outcome, oncology symptom clusters. According to the literature, patients receiving exclusively palliative care experience a distinct set of oncology symptoms compared to those in the early stages of the disease.10,11
For the sample size calculation, the patient population at the recruitment site and data from previous studies conducted at the same hospital were considered.¹⁰ The formula used for the sample size calculation was:
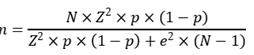
Where:
- n: calculated sample size;
- N: population size;
- Z: critical value corresponding to the desired confidence level;
- p: actual probability of the event;
- e: sampling error.11
The population considered for the sample size calculation included newly diagnosed patients at Afecc-Hospital Santa Rita de Cássia in 2022 (n = 3,513), a year unaffected by the bias caused by the COVID-19 pandemic. Additionally, the total number of new cancer cases in the state of Espírito Santo during the same period (n = 10,880) was also considered.12
Based on the inclusion and exclusion criteria, it was estimated that 20% of the newly diagnosed cases at Afecc-Hospital Santa Rita de Cássia would meet all eligibility criteria, resulting in 703 patients (20% of 3,513). This figure represents 6.45% of the new cancer cases reported in Espírito Santo between 2021 and 2022.
With a 95% confidence level (α = 5%), a 5% margin of error, and a test power of 80% (β = 0.20), the calculated sample size for this study was 84 patients.
Data collection, conducted between January and December 2023, utilized a sociodemographic and clinical questionnaire designed by the principal researcher. The questionnaire was developed based on an extensive literature review and the clinical-epidemiological variables included in the Tumor Registry Form from the hospital’s Cancer Hospital Registry (CHR).
Additionally, medical records were reviewed to gather detailed information on clinical and therapeutic aspects as well as blood count data.
The information collected in the questionnaire included: 1) sociodemographic data (including age, age group, self-reported ethnicity, gender, health region within the state of Espírito Santo, source of income, monthly income, education level, marital status, health insurance, and children); 2) medical history: past medical history and comorbidities; 3) clinical-epidemiological data: ICD-10 code, treatment type, histological type, TNM classification, clinical staging, current treatment and chemotherapy protocol, and time between diagnosis and treatment initiation.
To identify potential patients eligible for their first chemotherapy treatment, the schedules of clinical oncologists at the hospital were initially analyzed. After consultation with the clinical oncologist, patients were referred to the chemotherapy unit to schedule their first treatment cycle.
On the first day of chemotherapy, while the patient awaited infusion, an initial approach was made to invite them to participate in the study, following the eligibility criteria. During this interaction, the objectives of the study were explained, and the signature of the Informed Consent Form (ICF) was obtained.
Subsequently, before the chemotherapy infusion began, the sociodemographic and clinical questionnaire was administered, and medical records were reviewed to complement the collected information.
The study was approved by the Research Ethics Committee of the Health Sciences Center (CEP/CCS/UFES) under approval number 4122342.
Statistical analyses were performed using the R software (version 4.2.2) and RStudio (version 2023.03.1), with the significance level (α) set at 5%. Categorical variables were presented as absolute and relative frequencies, while numerical variables were described using measures of central tendency and dispersion.
RESULTS
Data from 84 oncology patients were analyzed. The mean age was 57.68 years (SD = ±11.81), with 42.86% (n = 36) falling within the 50–64 age group. The majority of patients were female, accounting for 72.62% (n = 61) of the sample. The most common self-reported ethnicity was mixed-race, representing 40.48% (n = 34), and most patients (88.10%, n = 74) resided in the metropolitan region of the state. Regarding income, 38.10% (n = 32) reported being retired, and 45% (n = 38) stated they earned the equivalent of one minimum wage. In terms of education, 48.81% (n = 41) indicated they had completed elementary school. Among marital statuses, the majority were married, comprising 51.19% (n = 43). Additionally, 25% (n = 21) of patients reported having four or more children, and 82.14% (n = 69) did not have private health insurance (Table 1).
Table 1. Sociodemographic characterization of oncology patients undergoing outpatient chemotherapy (n=84). Vitória (ES), Brazil, 2023.
|
Variable |
N |
% |
|
|
Age (in years) |
|
|
|
|
|
Mean (standard deviation) |
57,68 (11,81) |
- |
|
|
Median (interquartile range) |
58,00 (49,75 - 67,00) |
- |
|
Age group |
|
|
|
|
|
< 50 years |
21 |
25,00 |
|
|
50–64 years |
36 |
42,86 |
|
|
≥ 65 years |
27 |
32,14 |
|
Gender |
|
|
|
|
|
Male |
23 |
27,38 |
|
|
Female |
61 |
72,62 |
|
Self-reported ethnicity |
|
|
|
|
|
White |
32 |
38,10 |
|
|
Black |
10 |
11,90 |
|
|
Mixed-race |
34 |
40,48 |
|
|
Asian |
3 |
3,57 |
|
|
*No information |
5 |
5,95 |
|
Health regions of ES |
|
|
|
|
|
Metropolitan region |
74 |
88,10 |
|
|
Central-north region |
5 |
5,95 |
|
|
Southern region |
5 |
5,95 |
|
Source of income |
|
|
|
|
|
Retired |
32 |
38,10 |
|
|
Pensioner |
6 |
7,14 |
|
|
Employed |
19 |
22,62 |
|
|
No income |
20 |
23,81 |
|
|
Government beneficiary |
3 |
3,57 |
|
|
Self-employed |
4 |
4,76 |
|
Monthly income |
|
|
|
|
|
<1 minimum wage |
1 |
1,19 |
|
|
1 minimum wage |
38 |
45,24 |
|
|
Até 2 minimum wages |
13 |
15,48 |
|
|
Até 3 minimum wages |
10 |
11,90 |
|
|
*No information |
22 |
26,19 |
|
Education level |
|
|
|
|
|
Illiterate |
5 |
5,95 |
|
|
Elementary school |
41 |
48,81 |
|
|
High school |
29 |
34,52 |
|
|
Higher education |
1 |
1,19 |
|
Marital status |
|
|
|
|
|
Single |
15 |
17,86 |
|
|
Married |
43 |
51,19 |
|
|
Widowed |
11 |
13,10 |
|
|
Divorced |
11 |
13,10 |
|
|
Civil union |
4 |
4,76 |
|
Health insurance |
|
|
|
|
|
No |
69 |
82,14 |
|
|
Yes |
14 |
16,67 |
|
|
*No information |
1 |
1,19 |
|
Children |
|
|
|
|
|
None |
18 |
21,43 |
|
|
1 |
11 |
13,10 |
|
|
2 |
19 |
22,62 |
|
|
3 |
15 |
17,86 |
|
|
≥ 4 |
21 |
25,00 |
*No information: Data not collected.
Regarding comorbidities, 47.62% (n = 40) of patients had systemic arterial hypertension, 19.05% (n = 16) were diabetic, and 10.71% (n = 9) had dyslipidemia. Concerning family history of cancer, 66.67% (n = 56) reported cases of the disease among first- and second-degree relatives. Furthermore, 91.67% (n = 77) did not use tobacco, and 84.52% (n = 71) did not consume alcohol (Table 2).
Table 2. Medical history and comorbidities of oncology patients undergoing outpatient chemotherapy (n=84). Vitória (ES), Brazil, 2023.
|
Variable |
|
N |
% |
|
HAS* |
|
|
|
|
|
No |
44 |
52,38 |
|
|
Yes |
40 |
47,62 |
|
IAM† |
|
|
|
|
|
No |
80 |
95,24 |
|
|
Yes |
4 |
4,76 |
|
Dyslipidemia |
|
|
|
|
|
No |
75 |
89,29 |
|
|
Yes |
9 |
10,71 |
|
DM‡ |
|
|
|
|
|
No |
68 |
80,95 |
|
|
Yes |
16 |
19,05 |
|
Family History of Cancer |
|
||
|
|
No |
27 |
32,14 |
|
|
Yes |
56 |
66,67 |
|
|
**No information |
1 |
1,19 |
|
Tobacco Use |
|
|
|
|
|
No |
77 |
91,67 |
|
|
Yes |
5 |
5,95 |
|
|
**No information |
2 |
2,38 |
|
Alcohol Use |
|
||
|
|
No |
71 |
84,52 |
|
|
Yes |
11 |
13,10 |
|
|
**No information |
2 |
2,38 |
*HAS: Systemic Arterial Hypertension; †IAM: Acute Myocardial Infarction; ‡DM: Diabetes Mellitus; **No information: Data not collected.
Regarding clinical characteristics, malignant breast neoplasms predominated, representing 57.14% (n = 48) of cases, followed by malignant colon neoplasms at 22.62% (n = 19). The most common treatment was chemotherapy alone, performed on 57.14% (n = 48) of patients, followed by surgery combined with chemotherapy, accounting for 30.95% (n = 26). Among histological types, the most frequent were ductal carcinoma in situ (29.76%, n = 25) and adenocarcinoma (25%, n = 21). For TNM staging, the most common categories were T2N0M0 (27.38%, n = 23) and T2N1M0 (11.90%, n = 10). Regarding clinical staging, 57.14% (n = 48) of patients were in stage II, and 28.57% (n = 24) were in stage III. The most used chemotherapy protocol was adriamycin/cyclophosphamide (16.67%, n = 14), followed by docetaxel (13.10%, n = 11) (Table 3).
Table 3. Clinical characteristics of cancer patients undergoing outpatient chemotherapy (n=84). Vitória (ES), Brazil, 2023.
|
Variable |
N |
% |
|
|
CID-10 |
|
|
|
|
|
C18 – Malignant neoplasm of the colon |
19 |
22,62 |
|
|
C50 - Malignant neoplasm of the breast |
48 |
57,14 |
|
|
C54.1 – Malignant neoplasm of the endometrium |
1 |
1,19 |
|
|
C67 - Malignant neoplasm of the bladder |
2 |
2,38 |
|
|
C60 - Malignant neoplasm of the penis |
1 |
1,19 |
|
|
C34 - Malignant neoplasm of bronchus and lung |
5 |
5,95 |
|
|
C31.9 - Malignant neoplasm of nasal sinuses |
1 |
1,19 |
|
|
C160 - Malignant neoplasm of the cardia |
1 |
1,19 |
|
|
C44 - Undifferentiated malignant neoplasm (Merkel cell carcinoma) |
1 |
1,19 |
|
|
C22.1 - Cholangiocarcinoma |
1 |
1,19 |
|
|
C56 – Malignant neoplasm of the ovary |
1 |
1,19 |
|
|
C16 - Malignant neoplasm of the stomach |
1 |
1,19 |
|
|
C48 - Malignant neoplasm of soft tissues in the retroperitoneum and peritoneum |
1 |
1,19 |
|
|
C15 - Malignant neoplasm of the esophagus |
1 |
1,19 |
|
Treatment |
|
|
|
|
|
Chemotherapy |
48 |
57,14 |
|
|
Surgery + chemotherapy |
26 |
30,95 |
|
|
QT* + hormone therapy and radiotherapy |
1 |
1,19 |
|
|
Chemotherapy + radiotherapy |
3 |
3,57 |
|
|
Chemotherapy + surgery |
6 |
7,14 |
|
Histological Type |
|
|
|
|
|
Adenocarcinoma |
21 |
25,00 |
|
|
Ductal carcinoma in situ |
25 |
29,76 |
|
|
Invasive ductal carcinoma |
15 |
17,86 |
|
|
Invasive lobular carcinoma |
8 |
9,52 |
|
|
Others* |
15 |
17,86 |
|
TNM staging |
|
|
|
|
|
T1N0M0 |
7 |
8,33 |
|
|
T1N1M0 |
6 |
7,14 |
|
|
T1N2M0 |
1 |
1,19 |
|
|
T2N0M0 |
23 |
27,38 |
|
|
T2N1M0 |
10 |
11,90 |
|
|
T2N2M0 |
3 |
3,57 |
|
|
T2N3M0 |
1 |
1,19 |
|
|
T3N0M0 |
6 |
7,14 |
|
|
T3N1M0 |
3 |
3,57 |
|
|
T3N2M0 |
5 |
5,95 |
|
|
T3N3M0 |
2 |
2,38 |
|
|
T4N0M0 |
7 |
8,33 |
|
|
T4N1M0 |
5 |
5,95 |
|
|
T4N2M0 |
3 |
3,57 |
|
|
Sem informação |
2 |
2,38 |
|
Clinical staging |
|
|
|
|
|
I |
9 |
10,71 |
|
|
II |
48 |
57,14 |
|
|
III |
24 |
28,57 |
|
|
No information |
3 |
3,57 |
|
Current chemotherapy protocol |
|
|
|
|
|
Carboplatin / Paclitaxel |
6 |
7,14 |
|
|
Docetaxel / Cyclophosphamide |
8 |
9,52 |
|
|
Docetaxel |
11 |
13,10 |
|
|
Doxorubicin / Cyclophosphamide |
3 |
3,57 |
|
|
Adriamycin / Cyclophosphamide |
14 |
16,67 |
|
|
FOLFIRINOX / Leucovorin |
4 |
4,76 |
|
|
Docetaxel / Carboplatin |
3 |
3,57 |
|
|
FOLFIRINOX |
8 |
9,52 |
|
|
Fluorouracil / Leucovorin |
3 |
3,57 |
|
|
Others |
24 |
28,57 |
*QT: Chemotherapy; †Others: Cholangiocarcinoma; Poorly differentiated endometrial neoplasm; Squamous cell carcinoma of the right nasal cavity; Invasive squamous cell carcinoma of the penile glans; Locally advanced Merkel cell carcinoma; Non-invasive urothelial adenocarcinoma; High-grade papillary urothelial carcinoma of the bladder; Dedifferentiated liposarcoma and myxofibrosarcoma; Lung adenocarcinoma; Mucinous (colloid) carcinoma, grade II; Distal esophageal adenocarcinoma; Well-differentiated intramucosal gastric adenocarcinoma; Low-grade serous carcinoma; Poorly differentiated lung carcinoma, pathology suggests adenocarcinoma; Invasive squamous cell carcinoma.
Table 4 presents the results of the blood count analysis of cancer patients referred for outpatient chemotherapy.
Table 4. Blood count data of cancer patients undergoing outpatient chemotherapy (n=84). Vitória (ES), Brazil, 2023.
|
Variable |
Mean (standard deviation) |
Median (interquartile range) |
|
Red blood cells (million/mm3) |
4,30 (0,56) |
4,27 (3,94 - 4,60) |
|
Hemoglobin (g/dL) |
12,53 (1,69) |
12,60 (11,60 - 13,50) |
|
Hematocrit (%) |
37,47 (4,67) |
37,40 (35,30 - 40,50) |
|
M.C.V.* (fL) |
87,44 (6,80) |
88,18 (84,58 - 91,94) |
|
M.C.H.† (pg) |
29,26 (2,82) |
29,62 (27,80 - 31,19) |
|
M.C.H.C.‡ (g/dL) |
33,43 (1,21) |
33,42 (32,78 - 34,30) |
|
R.D.W.§ (%) |
13,51 (1,68) |
13,10 (12,50 - 14,10) |
|
R.D.W.|| (fL) |
42,74 (6,34) |
42,20 (40,10 - 44,70) |
|
White blood cells (thousand/mm3) |
7,38 (2,57) |
6,95 (5,78 - 8,25) |
|
Band neutrophils (%) |
2,03 (0,77) |
2,00 (1,00 - 3,00) |
|
Segmented neutrophils (%) |
66,36 (68,54) |
58,70 (52,50 - 64,40) |
|
Eosinophils (%) |
2,05 (1,48) |
1,90 (0,90 - 3,10) |
|
Basophils (%) |
0,49 (0,43) |
0,40 (0,20 - 0,60) |
|
Typical lymphocytes (%) |
28,46 (9,55) |
29,70 (23,70 - 33,40) |
|
Monocytes (%) |
8,00 (2,79) |
7,40 (6,00 - 9,40) |
|
Platelets (thousand/mm3) |
312,00 (108,47) |
294,00 (237,00 - 365,00) |
|
M.P.V.¶ (fL) |
10,45 (0,89) |
10,30 (9,80 - 11,10) |
*M.C.V.: Mean Corpuscular Volume; †M.C.H.: Mean Corpuscular Hemoglobin; ‡M.C.H.C.: Mean Corpuscular Hemoglobin Concentration; §R.D.W. (CV): Red Cell Distribution Width measured as coefficient of variation; ||R.D.W. (SD): Red Cell Distribution Width measured as standard deviation; M.P.V.: Mean Platelet Volume.
DISCUSSION
Most of the sample consisted of women, representing 72.62% of cases, aligning with the estimates from the National Cancer Institute (INCA) for the 2023–2025 period.5 The socioeconomic profile of the patients in this study reveals unfavorable living conditions, primarily reflected in low education levels and household income. Similarly, a study conducted with women diagnosed with breast cancer identified poor socioeconomic status, also associated with low income and education levels.6 Studies conducted in the Netherlands and Sweden support these findings, reporting lower breast cancer survival rates among women with lower education levels.13 Additionally, the Swedish study observed a higher frequency of early diagnoses in patients with higher educational attainment.13 These disparities in education and income are directly linked to access to cancer screening and early detection, factors that enable the implementation of more personalized and effective treatments.14
A study found a prevalence of 80.4% of married participants,15 whereas in the present sample, this percentage was 51.19%, with 21.43% of participants reporting no children. Although it is not possible to establish a direct relationship between the type of neoplasm and the number of children, these findings, combined with the fact that more than half of the participants were women, align with a population-based cohort study conducted in Lithuania. That study found that women with at least one child had a 16% lower risk of developing breast cancer, and multiparity was associated with an even greater reduction in risk.16 While the relationship between pregnancy, number of children, and breast cancer risk is complex,17 it is known that the carcinogenesis of this neoplasm is associated with genetic and environmental factors. Additionally, it is influenced by endocrine factors related to reproductive life, such as prolactin, estradiol, and progesterone levels.18
In this study, most patients (66.67%) reported a family history of cancer. Evidence indicates that a family history17 is significantly associated with an increased risk of developing cancer in adulthood, particularly in the presence of germline mutations.18
Although a minority of participants reported alcohol and tobacco use, these substances are directly linked to cancer development. Tobacco contains numerous carcinogenic compounds, while alcohol consumption increases the risk of cancers such as breast, liver, and esophageal cancer. This risk varies depending on the amount consumed, the type of alcoholic beverage, and other contributing factors.19
In line with the presented results, a study20 demonstrated that among more than 1,900 people who developed cancer over three years, 655 cases were breast cancer, followed by 330 cases of gastrointestinal neoplasms. Additionally, a cross-sectional study involving 4,140 nursing home residents in Europe21 revealed that 442 individuals (10.7%) had a cancer diagnosis. Among these, 56 patients had primary tumors, with breast cancer being the most prevalent, followed by non-melanoma skin cancer and colon cancer.
A retrospective cohort study conducted in South Korea found that 53.1% of diagnosed neoplasms were at pathological stages 1 and 2.15 Similarly, a study involving 83 patients diagnosed with small cell breast carcinoma showed that most cases were diagnosed at stage II, accounting for 33.7% of the sample.22
Regarding the therapeutic regimen, the findings of this study align with previous research15 that showed 30% of patients used a single antineoplastic agent, such as 5-fluorouracil (5-FU) or capecitabine. On the other hand, 70% underwent platinum-based therapies, such as FOLFOX (5-FU + oxaliplatin), XELOX (capecitabine + oxaliplatin), and paclitaxel + cisplatin. Additionally, 3.8% of the analyzed patients underwent extensive surgeries, including total gastrectomy, total colectomy, and pneumonectomy. Another investigation22 reported that 67.5% of patients received chemotherapy, 48.2% underwent radiotherapy, and more than half (55.4%) underwent breast-conserving surgery.
Cancer can cause inflammatory complications detectable at the serum level,20,23 but the main adverse effects are associated with chemotherapy toxicity. Common hematological changes include anemia, febrile neutropenia, thrombocytopenia, and leukopenia.24 However, blood count data collected in this study were obtained before the first cycle of chemotherapy began. As a result, the influence of treatment could not be observed, which explains the averages being within normal parameters.25
According to the World Health Organization (WHO),26 anemia is defined as a hemoglobin (Hb) concentration in the blood below the reference values: Hb <12 g/dL for women and Hb <13 g/dL for men. In this study, the mean hemoglobin level was 12.53 g/dL. Analyzing the interquartile range revealed that at least 25% of the sample had Hb levels of ≤11.60 g/dL. Thus, regardless of sex and respective reference values, at least 21 patients already exhibited anemia before the infusion of the first chemotherapy cycle.
Scientific evidence indicates that immune cells and their inflammatory actions within the tumor microenvironment directly influence cancer development and progression.23,27 Understanding the role of inflammation and the tumor microenvironment through the analysis of inflammatory response biomarkers is essential for defining patient prognosis and tailoring treatment appropriately.28 In this context, researchers have identified five inflammatory biomarkers associated with the clinical prognosis of oncology patients. These biomarkers are derived from combinations of blood parameters, such as neutrophils, lymphocytes, monocytes, and platelets.29 Regular monitoring of hematological changes via blood count analysis is crucial for assessing the effectiveness of therapeutic protocols and adjusting them as needed.24 This test, being minimally invasive and widely accessible, facilitates both cancer surveillance and treatment follow-up. It is often performed before and during therapy, enhancing patient care.30
A key limitation of this study is the inability to establish cause-and-effect relationships, a characteristic inherent to the cross-sectional design. Additionally, data collection and analysis were focused on the period prior to the first chemotherapy cycle, without addressing the progression of patients’ clinical conditions. Another limitation is that, as this study is part of a larger project excluding stage IV patients, it was not possible to capture the full range of clinical and epidemiological profiles. Despite these limitations, this research significantly contributes to understanding the clinical profile of non-metastatic cancer patients, providing valuable insights that can support strategies aimed at improving the follow-up care of these patients undergoing outpatient chemotherapy.
Another important limitation of the study was the absence of information due to some patients’ lack of responses. These data, categorized as “no information,” may have affected the completeness of the analyses, thereby limiting the generalizability of the results obtained.
CONCLUSION
The sociodemographic and clinical profile outlined in this study highlights the multifactorial, histological, and hematological complexity associated with cancer. To improve the prognosis of this disease, it is essential to go beyond the evaluation of sociodemographic and clinical variables by monitoring inflammatory biomarkers through blood count analysis during chemotherapy cycles. This approach promotes more effective patient management and follow-up care.
Understanding the clinical and epidemiological profile of oncology patients in treatment in Espírito Santo enables the identification of specific characteristics and risk factors within the population undergoing outpatient chemotherapy. These data can support efforts to improve analytical and non-analytical records in the Cancer Hospital Registry and guide the actions of healthcare professionals, particularly nurses working in chemotherapy outpatient clinics, fostering care that is more patient-centered and aligned with their needs and preferences. Furthermore, this study provides a foundation for future analytical research in other regions of Brazil, considering access issues and sociocultural aspects. It also contributes to planning cancer surveillance initiatives.
Finally, the identification of inflammatory biomarkers can enhance patient monitoring throughout chemotherapy cycles, contributing to the development of new care strategies and research initiatives in other regions of the country.
CONTRIBUTIONS
Study design or conception: Pessanha RM, Lopes-Júnior LC.
Data collection: Pessanha RM, Lopes-Júnior LC, D’Agostini NS, Giacomin LM, de Souza ANCV, Amaral MC, Busatto LS.
Data analysis and interpretation: Grippa WR, Pessanha RM, Lopes-Júnior LC.
Article writing or critical review: Grippa WR, Pessanha RM, Lopes-Júnior LC, D’Agostini NS, Giacomin LM, de Souza ANCV, Amaral MC, Busatto LS.
Final approval of the article version to be published: Lopes-Júnior LC.
CONFLICTS OF INTERESTS
The authors declare no conflicts of interest.
FUNDING
This research was funded by the Fundação de Amparo à Pesquisa e Inovação do Espírito Santo (FAPES) via FAPES Call No. 03/2021 – UNIVERSAL. Process number: 2021-5BDLS.
ACKNOWLEDGEMENTS
To Afecc-Hospital Santa Rita de Cássia for supporting this research.
REFERÊNCIAS
- Santos M de O, Lima FC da S de, Martins LFL, Oliveira JFP, Almeida LM de, Cancela M de C. Estimativa de Incidência de Câncer no Brasil, 2023-2025. Rev. Bras. Cancerol. [Internet]. 6º de fevereiro de 2023 [cited 2024 mar 6];69(1):e-213700. Available from: https://rbc.inca.gov.br/index.php/revista/article/view/3700
- Lopes-Júnior LC, Lima RAG. Cancer care and interdisciplinary practice. Cad Saúde Pública. 2019;35(1):e00193218. Portuguese. DOI: https://doi.org/10.1590/0102-311x00193218
- Lima RAG, Lopes-Júnior LC, Maia EBS, Fuentes-Alabi S, Ponce MLV. Global Initiative for Childhood Cancer Control: Increasing access, improving quality, saving lives. Rev Lat Am Enfermagem. 2023 Oct 6;31:e3998. DOI: https://doi.org/10.1590/1518-8345.0000.3998
- Ferlay J, Ervik M, Lam F, Laversanne M, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F (2024). Global Cancer Observatory: Cancer Today [Internet]. Lyon, France: International Agency for Research on Cancer. 2022 [cited 2024 mar 6]. Available from: https://gco.iarc.who.int/today
- Instituto Nacional de Câncer (Brasil). Estimativa 2023: incidência de câncer no Brasil / Instituto Nacional de Câncer. – Rio de Janeiro: INCA, 2022. Available from: https://www.inca.gov.br/publicacoes/livros/estimativa-2023-incidencia-de-cancer-no-brasil
- Marinho PML, Lima RB, Santos JC de O, Santos DK da C, Silva GM, Kameo SY, Sawada NO. Perfil Clínico-Epidemiológico e Qualidade de Vida Relacionada à Saúde de Mulheres com Câncer de Mama durante Tratamento Quimioterápico: Estudo Observacional. Rev. Bras. Cancerol. [Internet]. 12º de dezembro de 2022 [cited 2024 mar 7];68(4):e-253164. Available from: https://rbc.inca.gov.br/index.php/revista/article/view/3164
- Ministério da Saúde do Brasil Sistema de Informações Ambulatoriais do SUS (SIA) [Internet]. Rio de Janeiro, RJ: Ministério da Saúde. Available from: http://www.datasus.gov.br/
- Castro MC, Massuda A, Almeida G, Menezes-Filho NA, Andrade MV, de Souza Noronha KVM, et al. Brazil's unified health system: the first 30 years and prospects for the future. Lancet. 2019 Jul 27;394(10195):345-356. DOI: https://doi.org/10.1016/S0140-6736(19)31243-7
- Lopes-Júnior LC, Dell'Antonio LS, Pessanha RM, Dell'Antonio CS, da Silva MI, de Souza TM, Grassi J. Completeness and Consistency of Epidemiological Variables from Hospital-Based Cancer Registries in a Brazilian State. Int J Environ Res Public Health. 2022 Sep 22;19(19):12003. DOI: https://doi.org/10.3390/ijerph191912003
- Marcarini JAC, Grippa WR, Neto LCBS, Podestá OPG, Bolsoni-Lopes A, Nunes KZ, Lopes-Júnior LC. Nutritional status of women with non-metastatic breast cancer receiving outpatient chemotherapy. Nutrition. 2024 Jul;123:112411. DOI: https://doi.org/10.1016/j.nut.2024.112411
- Silva RJG, Grippa WR, Neto LCBS, Enriquez-Martinez OG, Marcarini JAC, Pessanha RM, Haraguchi FK, Lopes-Júnior LC. Factors Associated with the Nutritional Status of Women with Non-Metastatic Breast Cancer in a Brazilian High Complexity Oncology Center. Nutrients. 2023 Nov 29;15(23):4961. DOI: https://doi.org/10.3390/nu15234961
- Instituto Nacional de Câncer José Alencar Gomes da Silva. Estimativa 2020: incidência de câncer no Brasil / Instituto Nacional de Câncer José Alencar Gomes da Silva. – Rio de Janeiro: INCA, 2019. Available from: https://www.inca.gov.br/sites/ufu.sti.inca.local/files/media/document/estimativa-2020-incidencia-de-cancer-no-brasil.pdf
- Berglund A, Holmberg L, Tishelman C, Wagenius G, Eaker S, Lambe M. Social inequalities in non-small cell lung cancer management and survival: a population-based study in central Sweden. Thorax. 2010 Apr;65(4):327-33. DOI: https://doi.org/10.1136/thx.2009.125914
- Lopes-Júnior LC, Veronez LC. Personalized Care for Patients with Cancer in the Precision-Medicine Era. Int J Environ Res Public Health. 2023 Feb 9;20(4):3023. DOI: https://doi.org/10.3390/ijerph20043023
- Choi S, Seo S, Lee JH, Suh KJ, Kim JW, Kim JW, et al. Impact of Patient Sex on Adverse Events and Unscheduled Utilization of Medical Services in Cancer Patients Undergoing Adjuvant Chemotherapy: A Multicenter Retrospective Cohort Study. Cancer Res Treat. 2024 Apr;56(2):404-413. DOI: https://doi.org/10.4143/crt.2023.784
- Steponavičienė L, Vansevičiūtė R, Zabulienė L, Jasilionis D, Urbonas V, Smailytė G. Reproductive Factors and Breast Cancer Risk in Lithuanian Women: A Population-Based Cohort Study. Acta Med Litu. 2020;27(2):70-75. DOI: https://doi.org/ 10.15388/Amed.2020.27.2.4
- American Cancer Society. Cancer Facts & Figures 2022| American Cancer Society [Internet]. [cited 2024 mar 6]. Available from: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2022.html
- Flória-Santos M, Lopes-Júnior LC, Alvarenga Lde M, Ribeiro MS, Ferraz VE, Nascimento LC, Pereira-da-Silva G. Self-reported cancer family history is a useful tool for identification of individuals at risk of hereditary cancer predisposition syndrome at primary care centers in middle-income settings: a longitudinal study. Genet Mol Biol. 2016 Jun 3;39(2):178-83. DOI: https://doi.org/10.1590/1678-4685-GMB-2014-0362
- Lewandowska AM, Rudzki M, Rudzki S, Lewandowski T, Laskowska B. Environmental risk factors for cancer - review paper. Ann Agric Environ Med. 2019 Mar 22;26(1):1-7. DOI: https://doi.org/10.26444/aaem/94299
- Santaolalla A, Garmo H, Grigoriadis A, Ghuman S, Hammar N, Jungner I, et al. Metabolic profiles to predict long-term cancer and mortality: the use of latent class analysis. BMC Mol Cell Biol. 2019 Jul 23;20(1):28. DOI: https://doi.org/10.1186/s12860-019-0210-7
- Villani ER, Fusco D, Franza L, Onder G, Bernabei R, Colloca GF. Characteristics of patients with cancer in European long-term care facilities. Aging Clin Exp Res. 2022 Mar;34(3):671-678. DOI: https://doi.org/10.1007/s40520-021-01972-2
- Yin L, Yin A-H, Pu C-C. Clinical characteristics and prognosis of primary small cell carcinoma of the breast: a propensity score-matched, population-based study. BMJ Open 2023;13:e073841. DOI: https://doi.org/10.1136/bmjopen-2023-073841
- Kim JY, Jung EJ, Kim JM, Lee HS, Kwag SJ, Park JH, et al. Dynamic changes of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio predicts breast cancer prognosis. BMC Cancer. 2020 Dec 7;20(1):1206. DOI: https://doi.org/10.1186/s12885-020-07700-9
- Araújo DFB, Cavalcanti IDL, Larrazabal-Hadj-Idris BR, Peres AL. Hematological and biochemical toxicity analysis of chemotherapy in women diagnosed with cervical cancer. J Bras Patol Med Lab [Internet]. 2020;56:e1772020. Available from: https://doi.org/10.5935/1676-2444.20200038
- Celkan TT. What does a hemogram say to us? Turk Pediatri Ars. 2020 Jun 19;55(2):103-116. DOI: https://doi.org/10.14744/TurkPediatriArs.2019.76301
- World Health Organization. Nutritional anaemias: Tools for Effective Prevention and Control [Internet]. [cited 2024 Oct 13]. 2017. Available from: https://www.who.int/publications/i/item/9789241513067
- Jiang Y, Xu D, Song H, Qiu B, Tian D, Li Z, et al. Inflammation and nutrition-based biomarkers in the prognosis of oesophageal cancer: a systematic review and meta-analysis. BMJ Open. 2021 Sep 30;11(9):e048324. DOI: https://doi.org/10.1136/bmjopen-2020-048324
- Silva RJG, Grippa WR, Pessanha RM, Enriquez-Martinez OG, Neto LCBS, Lopes-Júnior LC. Neutrophil/Lymphocyte Ratio and Platelet/Lymphocyte Ratio and Their Relationship with Nutritional Status and Quality of Life of Hospitalized Women with Breast Cancer. Nutr Cancer. 2024;76(3):296-304. DOI: https://doi.org/10.1080/01635581.2024.2304689
- Boscolo-Rizzo P, D'Alessandro A, Polesel J, Borsetto D, Tofanelli M, Deganello A,et al. Different inflammatory blood markers correlate with specific outcomes in incident HPV-negative head and neck squamous cell carcinoma: a retrospective cohort study. BMC Cancer. 2022 Mar 5;22(1):243. DOI: https://doi.org/10.1186/s12885-022-09327-4
- Zhou JG, Wong AH, Wang H, Jin SH, Tan F, Chen YZ, et al. Definition of a new blood cell count score for early survival prediction for non-small cell lung cancer patients treated with atezolizumab: Integrated analysis of four multicenter clinical trials. Front Immunol. 2022 Sep 2;13:961926. DOI: https://doi.org/10.3389/fimmu.2022.961926
Correspondence
Prof. Dr. Luís Carlos Lopes-Júnior
E-mail: lopesjr.lc@gmail.com
Copyright© 2024 Revista de Enfermagem UFPE on line/REUOL.
Este é um artigo de acesso aberto distribuído sob a Atribuição CC BY 4.0 Creative Commons Attribution-ShareAlike 4.0 International License, a qual permite que outros distribuam, remixem, adaptem e criem a partir do seu trabalho, mesmo para fins comerciais, desde que lhe atribuam o devido crédito pela criação original. É recomendada para maximizar a disseminação e uso dos materiais licenciados.
 Português (Brasil)
Português (Brasil)  English
English  Español (España)
Español (España) 



















