
Idioma
Immunohistochemical biomarkers for high-grade squamous intraepithelial lesions of the cervix: a systematic review with meta-analysis
![]() Nirliane Ribeiro Barbosa1,
Nirliane Ribeiro Barbosa1, ![]() Luciana Xavier Pereira2,
Luciana Xavier Pereira2, ![]() Salviane dos Santos Barbosa3,
Salviane dos Santos Barbosa3, ![]() Anderson Ferreira Barbosa4,
Anderson Ferreira Barbosa4, ![]() Edilson Leite de Moura5,
Edilson Leite de Moura5, ![]() Elaine Virgínia Martins de Souza Figueiredo6,
Elaine Virgínia Martins de Souza Figueiredo6, ![]() Karol Fireman de Farias7,
Karol Fireman de Farias7, ![]() Teresinha Gonçalves da Silva8
Teresinha Gonçalves da Silva8
1,8Federal University of Pernambuco. Recife (PE), Brazil.
1,2,3,4,6,7Federal University of Alagoas. Arapiraca (AL), Brazil.
5Federal University of Alagoas. Maceió (AL), Brazil.
Introduction
Squamous intraepithelial lesions of the cervix are classified into low-grade squamous intraepithelial lesions (LSIL) and high-grade squamous intraepithelial lesions (HSIL). These lesions are associated with Human Papillomavirus (HPV), with subtypes 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, and 59 considered high-risk for oncogenic cancer. LSIL usually regresses; however, HSIL is considered a precursor to cervical cancer and can progress to carcinoma in situ if not treated appropriately. Cervical cancer is one of the leading causes of death in women worldwide, with some variations between countries and regions.1-4
To identify the characteristics of these lesions, histological assessment is necessary and, especially in cases of HSIL, assessment of immunohistochemical characteristics. Identifying these alterations and their characteristics is essential for the study of differential diagnoses and innovative therapeutic interventions, as several factors can contribute to a negative outcome in conization.3,5
Among the reasons that explain the absence of lesions on the cervix, the most frequent were colposcopy errors, spontaneous lesion regression, complete removal of small lesions during biopsy, errors in pre-conization material, false-negative results, and excisional error. Review of pathological specimen and the application of immunohistochemical biomarkers p16INK4 (or p16) and Ki-67 appeared to improve accuracy and help in the challenge of differential diagnosis.5 Thus, it is already well established that p16 and Ki-67 are surrogate biomarkers for the presence of HPV. However, there are reports of difficulties for pathologists in the differential diagnosis between cervical intraepithelial lesions, especially HSIL.6
For this purpose, the aim was to identify the main immunohistochemical markers for differentiating HSIL and to analyze the different methods of interpretation.
Method
This systematic review, registered in PROSPERO (International Prospective Register of Systematic Reviews) under number CRD420202107477, was conducted in March 2021 in the Cochrane, Embase, Scopus, and Web of Science databases using the following strategy: ((“Squamous Intraepithelial Lesions of the Cervix” OR “High-grade squamous intraepithelial lesion” OR “cervical intraepithelial neoplasia”) AND (“Biomarkers” OR “Marker” OR “inflammatory mediators” OR “inflammatory markers”) AND (“Histology” OR “Immunohistochemistry” OR “Immunofluorescence”)). The systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses protocol.8
This review aimed to answer the following question: what are the main immunohistochemical markers for differentiating HSIL and the different methods of interpretation? Descriptors were defined using the PICOS method,9 configuring the systematic review study, with Population (P): women with HSIL of the cervix; Intervention (I): immunohistochemical biomarker expression identification; Comparison or Control (C): women with LSIL in the cervix; Outcome (O): presence or absence of the association between immunohistochemical biomarker expression and HSIL of the cervix; Study Design (S): case-control, comparing immunohistochemical biomarker expression between HSIL and LSIL.
Original articles describing HSIL immunohistochemical biomarkers in cervical biopsies from 2000 to 2021 were included. Review articles, case reports, articles with animal studies, articles with in vitro studies, duplicate articles, and letters to the editor were excluded. Due to the secondary nature of the data collected and analyzed in the study, it was not submitted to a Research Ethics Committee.
Using the Rayyan platform, titles, abstracts, and full articles were assessed separately by two researchers to select studies for review, and in case of differences in selection between the two, a third researcher performed the assessment.
Two researchers independently extracted the data, carefully including them in the meta-analysis. The data collected were title, DOI, authors, year of publication, immunohistochemical biomarker, and immunohistochemical method for interpreting biomarker expression.
Meta-analysis was performed using Review Manager 5.3 software. For this purpose, the De Moura et al. method was used.10 Pooled Odds Ratio (OR) values with 95% Confidence Intervals (CI) were calculated to assess the association between immunohistochemical biomarker expression and HSIL of the cervix. Pooled ORs were determined by the Z-test, where a p-value <0.05 was considered significant.
The heterogeneity among studies was analyzed using the chi-square (Q2) and Higgins (I2) statistical tests.11 To calculate the pooled ORs, the fixed-effects model was used when p-value for heterogeneity was >0.05 or I2 < 50%, and the random-effects model was used when p-value for heterogeneity was <0.05 or I2 > 50%.12
This work was supported by the Alagoas State Research Support Foundation, through the Research Program for the Brazilian Health System 06/2016.
Results
A total of 157 articles emerged from the database search (Figure 1). These showed 130 biomarkers for HSIL of the cervix.

Figure 1 – Selection process for studies for systematic review and meta-analysis. Recife, PE, Brazil, 2023
The p16INK4 (or p16) biomarker was the most studied in HSIL of the cervix, present in 77 (55.79%) of the articles found. Subsequently, the Ki-67 biomarker appears in 34 (24.63%) of articles, followed by the other 128 biomarkers studied in up to seven (5.07%) of the articles resulting from the search. It is noteworthy that some articles studied more than one biomarker. For instance, 25 articles studied the p16 and Ki-67 biomarkers simultaneously.
Based on the most studied biomarkers in HSIL of the cervix, 57 articles were initially selected for this study. However, 53 articles were included, grouped according to the seven different immunohistochemical interpretation methods for p16 expression and three for Ki-67 expression: method “A” (nuclear or cytoplasmic staining by epithelial layers: no staining or focal staining = negative; diffuse staining = positive); method “B” (nuclear staining by epithelial layers: no staining = negative; focal and diffuse staining = positive); method “C” (staining by % of cells: 0% = negative; >0% = positive); method “D” (staining by % of cells: <1% of cells stained = negative; > or equal to 1% = positive); method “E” (staining by % of cells: <5% of cells stained = negative; > or equal to 5% = positive); method “F” (staining by %: <10% = negative; > or equal to 10% = positive); and method “G” (staining by %: < or equal to 25% = negative; > 25% = positive).
In addition to the different immunohistochemical interpretation methods mentioned, other methods were found that used more than one interpretation parameter and were therefore eliminated from this study.
P16 expression in cases of HSIL of the cervix was analyzed in 41 articles out of 53 included in this systematic review. These 41 articles were grouped into the seven different methods found in the studies, with 14 articles in method “A”, six in method “B”, three in method “C”, nine in method “D”, three in method “E”, four in method “F”, and two in method “G”.
Ki-67 expression in cases of HSIL of the cervix was analyzed in 12 articles out of 53 included in this study. These articles were grouped between two immunohistochemical interpretation methods found in the studies, with five articles using method “A”, five using method “F”, and two using method “G”.
The selection of outcome data for the meta-analysis was performed considering p16 and Ki-67 expression in cases of HSIL of the cervix compared to the control defined as LSIL in the cervix. This analysis was performed for each of the six immunohistochemical interpretation methods (from “A” to “F”) used to interpret p16 and/or Ki-67 expression individually. Only method “G” was not possible to generate a meta-analysis due to the insufficient number of studies. Thus, a total of 51 articles were included in the meta-analysis: 41 for p16 and ten for Ki-67.
Concerning the p16 biomarker, methods “A” and “D” were the most studied for immunohistochemical interpretation, while the meta-analysis reveals that method “A” represented the highest OR, with OR = 13.97 (95%CI: 7.93 - 24.63; Z = 9.12; p < 0.00001). This indicates that method “A” (nuclear or cytoplasmic staining by epithelial layers: no staining or focal staining = negative; diffuse staining = positive) is more efficient for interpreting p16 expression in HSIL and that women with positive p16 expression are 13.97 times more likely to develop HSIL compared to those with LSIL and those without positive p16 expression. Method “B” has an OR = 6.35 (95%CI: 4.18 – 9.65; Z = 8.67; p< 0.00001) for the p16 biomarker (Figure 2).
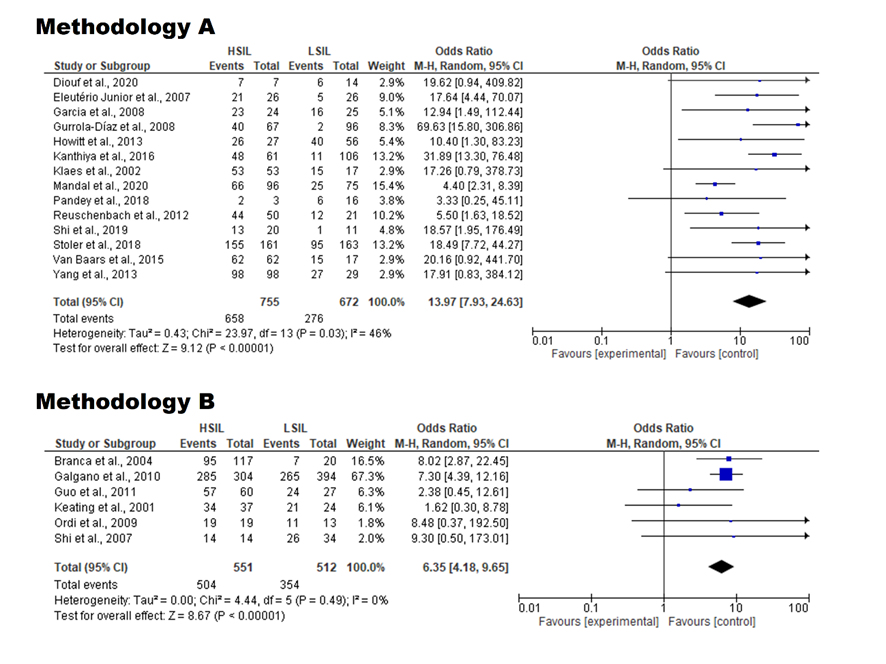
Figure 2 – Forest plots comparing methods “A” and “B” to interpret p16 expression in high-grade squamous intraepithelial lesions of the cervix. Recife, PE, Brazil, 2023
Figure 3 shows that method “C” has an OR = 5.06 (95%CI: 2.31 – 11.07; Z = 4.05; p< 0.0001) for the p16 biomarker, method “D” has an OR = 8.60 (95%CI: 3.71 – 19.72; Z = 5.02; p< 0.0001) and method “E” has an OR = 11.99 (95%CI: 2.80 – 51.34; Z = 3.35; p = 0.0008) for the p16 biomarker. Figure 4, in turn, shows that method “F” has an OR = 6.93 (95%CI: 2.92 – 16.45; Z = 4.39; p< 0.0001) for the p16 biomarker.
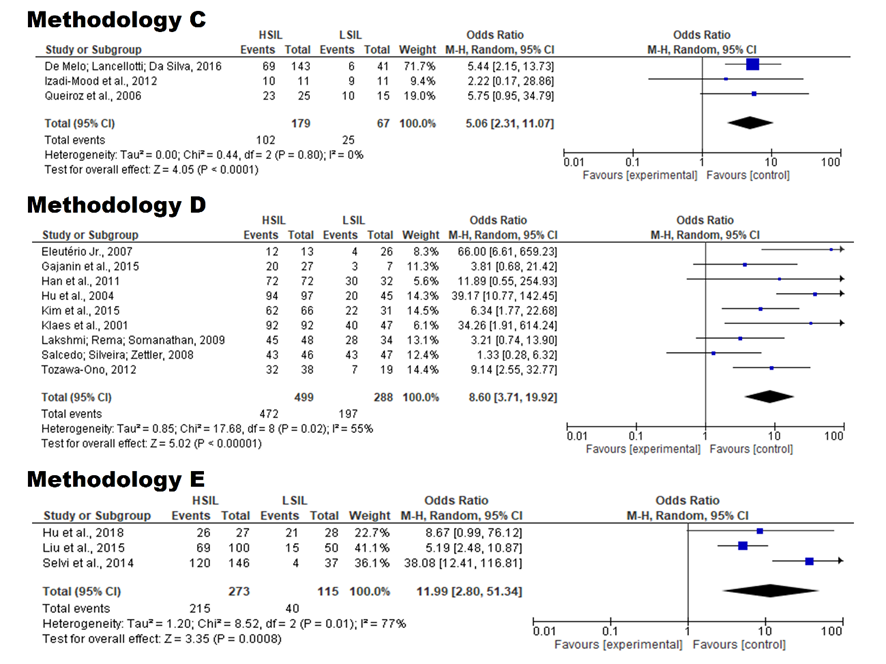
Figure 3 - Forest plots of comparisons that used methods “C”, “D”, and “E” to interpret p16 expression in high-grade squamous intraepithelial lesions of the cervix. Recife, PE, Brazil, 2023
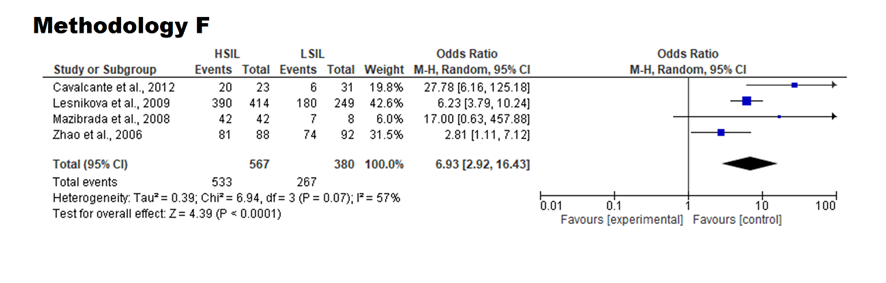
Figure 4 - Forest plots of comparisons that used the “F” method to interpret p16 expression in high-grade squamous intraepithelial lesions of the cervix. Recife, PE, Brazil, 2023
Methods “A” and “F” were equally studied for the Ki-67 biomarker (Figure 5), but the meta-analysis outcome reveals that method “A” represented the highest OR, with OR = 8.47 (95%CI: 3.75 – 19.14; Z = 5.13; p < 0.00001). This indicates that method “A” is also more efficient for interpreting Ki-67 expression in HSIL, and that women with positive Ki-67 expression are 8.47 times more likely to develop HSIL compared to LSIL, when compared to those without positive Ki-67 expression. Figure 5 also shows that method “F” has an OR = 6.44 (95%CI: 2.11 – 19.66; Z = 3.27; p = 0.001) for the Ki-67 biomarker.
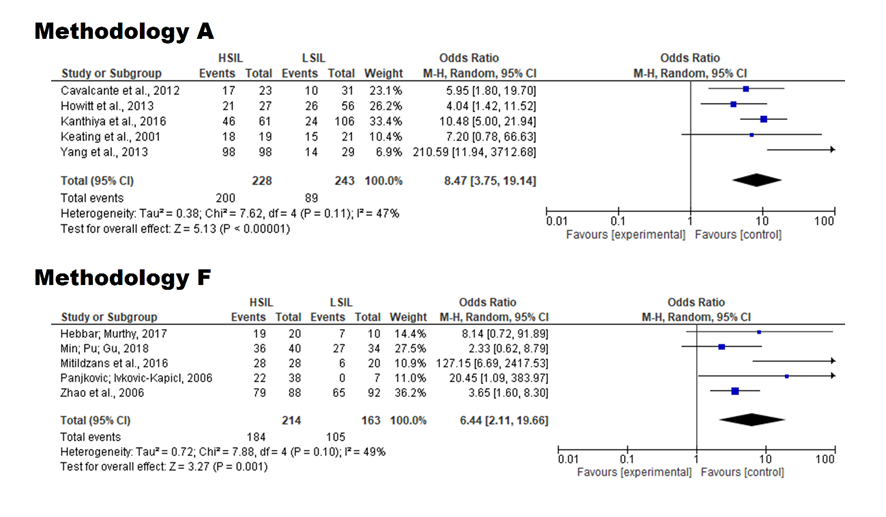
Figure 5 - Forest plots of comparisons that used methods “A” and “F” to interpret Ki-67 expression in high-grade squamous intraepithelial lesions of the cervix. Recife, PE, Brazil, 2023
Furthermore, heterogeneity was found in 14 comparisons that used method “A” to interpret the p16 expression (I2 = 47%; P = 0.03). On the other hand, in five comparisons of Ki-67 expression interpretation using method “A”, no heterogeneity was detected (I2 = 47%; P = 0.11).
Discussion
Given the difficulty in differential diagnosis between cervical lesions based solely on morphology, immunohistochemistry (IHC) becomes an alternative to be applied for the identification of specific biomarkers for each type of lesion.13 In clinical practice, IHC has already been widely used for different types of cancer, and many studies have indicated the importance of its application not only for diagnosis but also for the indication of personalized therapies.14
This systematic review indicates that p16 and Ki-67 are the main biomarkers for HSIL of the cervix. In fact, biomarkers are more effective in confirming the presence of major anomalies, such as HSIL, than minor alterations such as LSIL.13 Several studies have already highlighted the strength of the expression of these two biomarkers in HSIL of the cervix. P16 expression has been widely applied and studied in HSIL of the cervix diagnosis, while, secondarily, Ki-67 expression has also proven important for this diagnosis.15-20
These results may be related to HSIL pathogenesis, because although LSIL and HSIL are related to HPV infection, HSIL has been identified as being associated with high-risk HPV types, while LSIL mainly presents with low-risk HPV. One of the most common high-risk HPV types found among HSIL patients is HPV-16, whose greater persistence in the body increases the chances of progression to malignant neoplasms due to the production of oncogenes such as E7.21-24
To understand the relationship between p16 and Ki-67 expression and HSIL pathogenesis, it is necessary to consider the biology of the cell cycle. The p16 protein (also known as p16INK4A) is a tumor suppressor protein that regulates cell cycle progression by inhibiting cyclin-dependent kinases, more specifically CDK4/6. This inhibition prevents the phosphorylation of retinoblastoma protein (pRB), which then continues to block the transcription factor E2F, preventing the transcription of genes related to cell cycle progression.25 In HPV-16 infection, the viral oncoprotein E7 is produced, which binds to pRB, inactivating it, and E2F is released and then acts on the expression of genes that will lead to cell cycle progression. Consequently, p16 is upregulated, resulting from a negative feedback mechanism in the cell.26
Furthermore, as a consequence of the deregulated cell cycle progression resulting from the action of the viral oncoprotein E7, there will be an increase in the number of mitoses. Ki-67 is a nuclear protein present in the cell cycle phases, and is therefore used as a marker of cell proliferation for the investigation of neoplasm diagnoses. The importance of histopathological assessment using hematoxylin and eosin together to assess the presence of atypical mitoses is highlighted.13;27
Therefore, the diffuse p16 and Ki-67 expression is associated with HSIL pathogenesis, which is related to the prevalence of high-risk HPV and, thus, greater action of the E7 oncogene. This leads to cell cycle dysregulation, with consequent overexpression of p16, resulting from the negative feedback mechanism of the cell, as described previously, and also an increase in Ki-67 expression, resulting from the increased number of mitoses, when compared to LSIL.
A recent review study demonstrated the clinical importance of cervical cancer screening, emphasizing the need for and success of different tools that precisely guide clinical decision-making and the correct treatment for patients, such as dual labeling for p16/ki67.28 Furthermore, other recent studies have shown the role of IHC for p16 and ki67 in distinguishing between HSIL and LSIL.29-31 However, this study is the first systematic review with meta-analysis to rigorously demonstrate the relationship between the expression of these biomarkers as a complementary tool in the differential diagnosis of HSIL.
It is important to highlight that, in this systematic review, it was observed that immunohistochemical diagnosis for HSIL of the cervix has been performed using a variety of methods for analyzing tissue staining, with up to seven different immunohistochemical interpretation methods identified for interpreting p16 and Ki-67 expression. This result indicates a lack of standardization in this type of analysis, which may interfere with the final diagnosis. The study showed that difficulties still exist in the interpretation of IHC staining, especially for p16.19 Therefore, for the meta-analysis, subgroups were established according to the immunohistochemical interpretation method used on the extracted data, with the aim of reducing the influence of this factor on the heterogeneity of the effect size among studies.
Although all subgroup analyses showed a positive relationship between the presence of biomarkers and HSIL, it is noted that even different immunohistochemical interpretation methods with similar classification present an important difference in the reading of biomarker expression. Among the methods found, method “A”, using nuclear or cytoplasmic staining by epithelial layers (no staining or focal staining = negative; diffuse staining = positive), shows greater significance for interpreting p16 expression in HSIL, with the highest OR among the subgroups analyzed (OR = 13.97; 95%CI: 7.93 - 24.63; Z = 9.12; p < 0.00001), when compared to LSIL. Similarly, this method showed greater significance for interpreting the Ki-67 biomarker, with a higher OR (OR = 8.47; 95%CI: 3.75 – 19.14; Z = 5.13; p<0.00001). Therefore, method “A”, which considers nuclear or cytoplasmic staining by epithelial layers, with no staining or focal staining considered negative and diffuse staining considered positive, showed the highest OR. This result indicates that the IHC analysis method can increase the chances of identifying clinical cases of HSIL and thus influence patient decision-making.
Some limitations of this systematic review and meta-analysis relate to the inclusion of only immunohistochemical biomarkers, but there are other markers to be studied in this context, such as immunological and genetic markers. Furthermore, the study design resulted in a prolonged time for data search, analysis, and interpretation. Therefore, it is possible that recent articles were not included in this review and meta-analysis.
Conclusion
HSIL diagnosis in the cervix can be made using different methods. To ensure the clinical safety of women, it is essential to follow scientific evidence with specific criteria. This systematic review with meta-analysis contributes to the validation of p16 and Ki-67 biomarkers as the most relevant in HSIL histopathological diagnosis compared to LSIL. Furthermore, it describes the different methods for interpreting p16 and Ki-67 expression, indicating that the method that classifies nuclear or cytoplasmic staining by epithelial layers (no staining or focal staining = negative; diffuse staining = positive) is more significant for interpreting both biomarkers in HSIL.
Authors’ contributions
Nirliane Ribeiro Barbosa: study elaboration; data collection; data analysis and interpretation; manuscript writing; approval of the final version of the text. Luciana Xavier Pereira: study elaboration; data collection; data analysis and interpretation; manuscript critical writing; approval of the final version of the text. Salviane dos Santos Barbosa: data collection. Anderson Ferreira Barbosa: data collection. Edilson Leite de Moura: data analysis and interpretation; manuscript critical review; final approval of the manuscript. Elaine Virgínia Martins de Souza Figueiredo: manuscript critical review; final approval of the manuscript. Karol Fireman de Farias: manuscript critical review; final approval of the manuscript. Teresinha Gonçalves da Silva: manuscript critical review; final approval of the manuscript.
Conflict of interest
The authors declare that they received financial support from the Alagoas State Research Support Foundation, without the funding source having participated in the preparation of this article. There are no other financial interests or personal relationships that could be considered potential conflicts of interest.
Financing
Research Support Foundation of the State of Alagoas, through the Research Program for the Brazilian Health System 06/2016.
Acknowledgments
The authors thank the Alagoas State Research Support Foundation for its financial support. Furthermore, they express their gratitude to physician and professor Hamilton Pimentel dos Santos Filho for his contribution to the content review.
References
1. Brasil. Ministério da Saúde. Secretaria de ciência, tecnologia, inovação e do complexo econômico-industrial da saúde [Internet]. Portaria conjunta SAES/SECTICS NO 13, de 29 de julho de 2025. Aprova as Diretrizes Brasileiras para o Rastreamento do Câncer de Colo do Útero: Parte I – Rastreamento organizado utilizando testes moleculares para detecção de DNA-HPV Oncogênico. 2025. Avaliable from: https://www.gov.br/inca/pt-br/assuntos/noticias/2025/aprovada-diretrizes-brasileiras-para-o-rastreamento-do-cancer-de-colo-do-utero.
2. Manga SM, Ye Y, Nulah KL, Manjuh F, Fokom-Domgue J, Scarinci I, et al. Human papillomavirus types and cervical cancer screening among female sex workers in Cameroon [Internet]. Cancers. 2024;16: 1-17. DOI: https://doi.org/10.3390/cancers16020243.
3.World Health Organization [Internet]. Guideline for screening and treatment of cervical pre-cancer lesions for cervical cancer prevention. 2021. Avaliable from: https://www.who.int/publications/i/item/9789240030824/.
4. Zanine RM. Doenças do Trato Genital Inferior e Colposcopia: um enfoque na terapêutica. 1 ed. Rio de Janeiro: Thieme Revinter; 2021.
5. Lorenset LC, Zanine RM. Reliability of negative cone specimens of the cervix: A review [Internet]. Ann Diagn Pathol. 2022. DOI: https://doi.org/10.1016/j.anndiagpath.2022.151929
6. Melo CAF, Utagawa ML. Expressão imuno-histoquímica dos biomarcadores p16 e Ki-67 na lesão intraepitelial cervical de alto grau: revisão de estudos [Internet]. RBAC. 2021;53 (3): 228-231. DOI: https://doi.org/10.21877/2448-3877.202202030
7. Barbosa NR, Pereira, LX, Farias KF, Silva TG, 2020. High-grade squamous intraepithelial lesion in uterine cervix: a systematic review with meta-analysis [Internet]. International prospective register of systematic reviews/ PROSPERO.1-12. Avaliable from: https://www.crd.york.ac.uk/PROSPERO/view/CRD42020210747.
8. Galvão TF, Tiguman GMB, Sarkis-Onofre R. A declaração PRISMA 2020 em português: recomendações atualizadas para o relato de revisões sistemáticas [Internet]. Epidemiol. Serv. Saúde. 2022;31(2). DOI: https://doi.org/10.1590/SS2237-9622202200011.
9. Roever L, Gomes-Neto M, Durães AR, Reis PEO, Pollo-Flores P, Silva RML, Resende ES. Compreendendo o GRADE: PICO e qualidade de estudos [Internet]. Rev Soc Bras Clin Med. 2021;19 (1):54-61. Avaliable from: https://docs.bvsalud.org/biblioref/2022/03/1361752/54-61.pdf.
10. De Moura EL, Dos Santos ACM, Da Silva DM, Dos Santos BB, Figueredo DS, Moura AWA, et al. Association of polymorphisms in cytokine genes with susceptibility to precancerous lesions and cervical cancer: a systematic review wiht meta-analysis [Internet]. Immunol Invest. 2020;50:492-526. DOI: https://doi.org/10.1080/08820139.2020.1778023.
11. Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis [Internet]. Stat Med. 2002;21:1539-58. DOI: https://doi.org/10.1002/sim.1186.
12. Dersimonian R, Laird N. Meta-analysis in clinical trials [Internet]. Controlled Clinical Trials. 1986;7:177-188. DOI: https://doi.org/10.1016/0197-2456(86)90046-2.
13. Kamal M. Pré-cânceres cervicais: biópsia e imuno-histoquímica [Internet]. CytoJournal. 2022;19 (38):1-17. DOI: https://doi.org/10.25259/CMAS_03_13_2021.
14. Mebratie DY, Dagnaw GG. Revisão de técnicas de imunohistoquímica: aplicações, estado atual e perspectivas futuras [Internet]. Seminars in Diagnostic Pathology. 2024;41(3):154-160. DOI: https://doi.org/10.1053/j.semdp.2024.05.001.
15. Bittencourt DD, Zanine RM, Ribas CAPM, Czeczko NG, Tabushi FI. Avaliação epidemiológica e expressão dos marcadores P16/Ki-67 como fatores de risco na persistência ou recidiva da lesão intraepitelial de alto grau [Internet]. Scielo preprints. 2022. DOI: https://doi.org/10.1590/SciELOPreprints.4132.
16. Dovnik A, Repše Fokter A. O papel da coloração dupla p16/Ki67 no rastreamento do câncer cervical [Internet]. Curr. Issues Mol. Biol. 2023;45:8476–8491. DOI: https://doi.org/10.3390/cimb45100534.
17. Zuberi Z, Mremi A, Chilongola JO, Semango G, Sauli E. Análise da expressão dos biomarcadores proteicos p16 e TOP2A em lesões de câncer cervical e sua correlação com características clínico-histopatológicas em um hospital de referência, Tanzânia [Internet]. PLoS ONE. 2021;16(10):e0259096. DOI: https://doi.org/10.1371/journal.pone.0259096.
18. Ding L, Song L, Zhao W, Li X, Gao W, Qi Z, Wang J. Valor preditivo das características imunoqualitativas de p16INK4a, Ki-67 e ProExC na progressão de LSIL para HSIL [Internet]. Exp Ther Med. 2020;19:2457-2466. DOI: https://doi.org/10.3892/etm.2020.8496
19. Liu J, Su S, Liu Y. O valor do Ki67 para o diagnóstico de LSIL e os problemas do p16 no diagnóstico de HSIL [Internet]. Sci Rep. 2022;12:7613. DOI: https://doi.org/10.1038/s41598-022-11584-z.
20. Feitoza EN, Oliveira D de O, Carvalho BM, Andrade ML. Diagnóstico precoce do câncer de colo do útero utilizando biomarcadores tumorais P16 e Ki67: uma revisão sistemática [Internet]. Braz. J. Hea. Rev. 2023;6(3):13881-90. DOI: https://doi.org/10.34119/bjhrv6n3-427.
21. Tao X, Austin M, Yu T, Zhong F, Zhou X, Cong C et al. Estratificação de risco para neoplasia cervical usando genotipagem estendida de HPV de alto risco em mulheres com citologia ASC-US: um grande estudo retrospectivo da China [Internet]. Cancer Cytopathology. 2022;130(4):248-252. DOI: https://doi.org/10.1002/cncy.22536.
22. Luo Q, Zeng X, Luo H, Pan L, Huang Y, Zhang H, Han N. Características epidemiológicas do HPV de alto risco e a correlação entre infecções múltiplas e lesões cervicais [Internet]. Doenças Infecciosas BMC. 2023;23(667):1-14. DOI: https://doi.org/10.1186/s12879-023-08634-w.
23. Liu Q, Chen L, Yu M, Zhou X, Zhang X, Zheng W, Niu S, Zhou F. Prevalência de pré-cânceres ou cânceres cervicais em mulheres com citologia ASC-H/HSIL de acordo com os genótipos de HPV detectados pelo ensaio Aptima HPV (AHPV) e idade [Internet]. J Câncer. 2024;15(1):140-148. DOI: https:doi.org/10.7150/jca.89715.
24. Khieu M, Butler SL. High-Grade Squamous Intraepithelial Lesion of the Cervix. [Updated 2023 Nov 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430728/
25. Serrano M, Hannon GJ, Beach D. A new regulatory motif in cell·cycle control causing specific inhibition of cyclin D/CDK4 [Internet]. Nature. 1993;366:704-707. DOI: https://doi.org/10.1038/366704a0.
26. Khleif SN, DeGregori J, Yee CL, Otterson GA, Kaye FJ, Nevins JR, Howley PM. A inibição da atividade da ciclina D-CDK4/CDK6 está associada à indução mediada por E2F da atividade inibidora da ciclina quinase [Internet]. Proc. Natl. Acad. Sci. EUA. 1996;93:4350-4354. DOI: https://doi.org/10.1073/pnas.93.9.4350.
27.Sun X, Kaufman PD. Ki-67: mais que um marcador de proliferação [Internet]. Chromosoma. 2018;127:175–186. DOI: https://doi.org/10.1007/s00412-018-0659-8.
28. Perkins RB, Wentzensen N, Guido RS, Schiffman M. Rastreamento do câncer Cervical: uma revisão [Internet]. JAMA. 2023;330(6):547-558. DOI: https://doi.org/10.1001/jama.2023.13174.
29. Hosseini MS, Talayeh M, Moghaddam NA, Arab N, Farzaneh F, Ashrafganjoei T. Comparação do índice Ki67 e da expressão de P16 em diferentes graus de lesões intraepiteliais escamosas cervicais [Internet]. Caspian J Intern Med. 2023;14(1):69-75. DOI: https://doi.org/10.22088/cjim.14.1.69.
30. Wu M, Wang SY, Zheng M, Tian LX, Wu X, Guo K, Zhang Y, Wu G. A utilidade diagnóstica da imunocoloração p16 na diferenciação de câncer e HSIL de LSIL e benigno em células cervicais [Internet]. Transplante celular. 2019;28(2):195-200. DOI: https://doi.org/10.1177/0963689718817478.
31. Silva DC, Gonçalves AK, Cobucci RN, Mendonça RC, Lima PH, Júnior GC. Expressão imuno-histoquímica de p16, Ki-67 e p53 em lesões cervicais – Uma revisão sistemática [Internet]. Pathology – Research and Practice. 2017;213(7):723–729. DOI: https://doi.org/10.1016/j.prp.2017.03.003.Silva DC, Gonçalves AK, Cobucci RN, Mendonça RC, Lima PH, Júnior GC. Expressão imuno-histoquímica de p16, Ki-67 e p53 em lesões cervicais – Uma revisão sistemática [Internet]. Pathology – Research and Practice. 2017;213(7):723–729. DOI: https://doi.org/10.1016/j.prp.2017.03.003.
Corresponding Author
Name: Nirliane Ribeiro Barbosa
E-mail: nirliane.barbosa@ufpe.br
© The Author(s) 2025. This work is licensed under Creative Commons Attribution 4.0 International. License text for use: https://creativecommons.org/licenses/by/4.0/
 Português (Brasil)
Português (Brasil)  English
English  Español (España)
Español (España) 



















