
Idioma
Barriers to the implementation of nursing actions aimed at preventing alcohol use among indigenous populations
Nunes DAS, Gallo AM, Marques FRDM, Santos GA dos, Dias LE, Salci MA, Carreira L.
INTRODUCTION
The indigenous population reached 1,693,535 people in 2022, representing 0.83% of the general population and an increase of 88.82% compared to the 2010 census. Most of this population is concentrated in the states of Amazonas and Bahia, 490,900 and 229,100 respectively, followed by Mato Grosso do Sul (116,300), Pernambuco (106,600) and Roraima (97,300).1 The Guarani are one of the largest indigenous populations in South America. They are ancestral inhabitants of the coast and central region of Brazil and are divided into three subgroups: Mbya, Ñandeva, and Kaiowá, with the latter two subgroups occupying areas in the state of Mato Grosso do Sul. Their way of life involves natural, social, and cosmological factors and their ancient and present teachings indicate the way these peoples live.2
Brazil's indigenous populations have faced problems arising from the problematic use of alcohol in their territories since the beginning of the expansionist processes. Harmful and harmful use of alcohol are essential concepts in assessing patterns of consumption of this substance and identifying possible problems related to its use. In this sense, harmful use is characterized by a pattern of consumption that causes damage to physical or mental health, without, however, meeting the criteria for a diagnosis of alcohol dependence. Harmful use involves a pattern of consumption that also causes damage to physical or mental health, but meets the criteria for a diagnosis of alcohol dependence, which includes serious physical or mental health problems, impairment of social relationships, and legal and occupational problems, among others.3
In Indigenous populations, the use of alcohol can be related to the process of Indigenous acculturation4 and the loss of traditional identity references, as well as changes in lifestyles caused by urbanization and precarious living and health conditions. It's a complex issue that requires a specific approach that incorporates the concepts mentioned above, the way of living and dealing with problems from the Guarani point of view.5 In this sense, it is fundamental to look for concepts about the processes of alcoholization to rethink alcoholism and highlight the varied consequences of alcohol consumption in minority groups such as indigenous peoples.6
This approach sheds light on the meaning of the harmful use of alcohol, identifies the rules and norms that permeate consumption, as well as its transgressions, and, when standardized according to the specificities of Indigenous people, does not allow for generalization or approximation of the ways of drinking to what is standard for non-indigenous society. In this way, screening instruments such as the Alcohol Use Disorders Identification Test (AUDIT) and the CAGE Questionnaire3 used by health professionals to identify consumption patterns and assess alcohol consumption, risk behaviors, and health problems related to its use, are not suitable for the Indigenous context, if applied in a way that is decontextualized from the reality of Indigenous peoples.7
In addition, the National Policy for the Health Care of Indigenous Peoples (NPHCIP) and the Indigenous Health Care Subsystem (IHCS) have the prerogative of guaranteeing access to quality health services while respecting indigenous peoples' cultural and territorial specificities. In the context of harmful use, it is important to consider that alcohol affects not only health but also social and environmental aspects. It is up to health policies to incorporate coping actions through integration with other public policies that address broader social issues and that characterize vulnerability in the living conditions of Indigenous peoples, such as unemployment, poverty, and access to health and education, as they are the result of multidimensional factors that require efforts from different spheres to tackle.5
Brazil has faced the challenge of harmful alcohol use for decades, with social, economic, and health impacts, as well as serving as a gateway to the use of other Psychoactive Substances (PASs). To deal with this issue, the country implemented the Dry Law, which prohibits alcohol consumption by drivers, resulting in a significant reduction in alcohol-related traffic accidents. In the indigenous context, decree no. 2.759 introduced the guidelines for the National Policy for Comprehensive Care for Indigenous Mental Health8. However, the actions are mainly concentrated in primary care and point to important challenges, such as the shortage of professionals and difficulties in accessing health services.9
Alcohol consumption in Indigenous territories is associated with social and health determinants, and the reality of the consumption of these substances in Indigenous territories, as well as their real consequences, are priorities on the political agenda of the Millennium Sustainable Development Goals (SDGs).10
SDG goal number three (SDG 3) aims to “ensure healthy lives and promote well-being for all at all ages”. This goal is quite comprehensive and includes several specific targets. Among the main targets is the need to strengthen the prevention and treatment of substance abuse, i.e. including drug and narcotic abuse and harmful use of alcohol.10 In this context, nursing professionals take on a prominent role, as they are on the front line of the fight against drug use, providing education, prevention, treatment, and rehabilitation for those struggling with the harmful use of alcohol.11
In addition, nurses are part of multidisciplinary Indigenous health teams linked to the Special Indigenous Health Districts (SIHD), which are responsible for PHC in Indigenous territories. In this way, they play their part in promoting health and preventing diseases related to the harmful use of alcohol through educational actions, with cultural approaches that seek to understand the problems arising from alcohol consumption and care through direct assistance to Indigenous people who need outpatient care, home visits, and case follow-up.2
It is worth noting that nurses play a key role in the care of indigenous populations, mediating the relationship between the health system and the communities. They work to train indigenous health workers, participate in the creation of prevention strategies, and are often the professionals closest to these communities, in addition to building a relationship of trust and strengthening the bond between professional and patient.11
In the indigenous context, nursing professionals are faced with the challenge of entering communities with important cultural specificities. Part of this problem could be solved in the training of professionals themselves, if their trainers brought them closer to the contexts of vulnerable populations, such as indigenous peoples.
Thus, the challenge for nursing professionals when working with indigenous populations is, firstly, to understand and integrate with the specific knowledge and ways of life of each ethnic group, which has its own beliefs and worldviews.12
In addition, alcohol consumption represents a significant challenge for indigenous populations, and nursing professionals working in these territories face various barriers when dealing with this issue. In many communities, alcohol is an easily accessible substance and its consumption is rooted in cultural and social practices. It is important to reiterate that contact with non-indigenous society made it possible to introduce alcohol into these communities, incorporating a new style of consumption of this substance. The effects of the harmful use of alcohol are those observed in the non-indigenous population, i.e. physical and mental health problems, domestic violence, accidents, and family disintegration.8
It is still a challenge for nursing in Indigenous contexts to understand the root causes of this behavior, which are often associated with socioeconomic and historical issues that permeate relations between Indigenous and non-indigenous populations. In addition, the lack of resources and the insipid nature of specific policies to deal with the harmful use of alcohol in Indigenous communities make it even more difficult for these professionals to work in the territories.11
Although there are public policies aimed at Indigenous health, few studies have specifically addressed the cultural and structural barriers that hinder the prevention of alcohol use in these communities. These few studies have pointed to the need to understand the processes of alcoholization in Indigenous communities from introspection into Indigenous knowledge about the problem of alcohol use in their communities and their coping strategies, taking into account the social heritage of these ancient communities.5,6
Thus, knowing how nurses and nursing technicians carry out preventive actions aimed at the harmful use of alcohol in Indigenous populations, as well as identifying the obstacles to carrying out these actions, can contribute to improving nursing practice in Indigenous communities, and promoting more humanized, culturally sensitive, and evidence-based interventions.
The question arose from the gap between the nursing care provided to the Indigenous population and the challenges and barriers that exist in this territory regarding the harmful use of alcohol, and the urgent need to meet the global goals of the United Nations (UN) that “no one be left behind”: What are the main obstacles that hinder the implementation of nursing actions aimed at preventing the use of alcohol in Indigenous populations?
OBJECTIVE
To identify the obstacles to the implementation of nursing actions aimed at preventing alcohol use in indigenous populations.
METHOD
The research was conducted by a single researcher, a nurse, and a professor of higher education with 15 years of experience in health care for indigenous populations. Despite the researcher's closeness to one of the nursing teams interviewed, a brief initial interaction took place to explain the objectives of the research and obtain consent to take part in the study. Reflexivity was maintained throughout the process, with the researcher documenting her impressions and reflections after each interview.
This is a descriptive study with a qualitative approach,13 which used transcultural care for Indigenous people as its theoretical framework, anchored in the contributions of Madeleine Leininger's Diversity and Universality Theory of Cultural Care,14 as it allows us to understand how social and cultural structures influence the state of health, well-being or illness.
The methodological framework was guided by the premises of narrative research, which is characterized by the combination of characters and events in the reported speeches, and that the narrated, subjective, and/or intersubjective stories have an impact on the listener due to their similarity to real life.15 Content Analysis was used to systematically structure the data.16
The study participants were selected intentionally and were nursing professionals working in Indigenous health. The selection criteria were: 1) being a nursing professional working in Indigenous health for more than 12 months and regardless of how long they had been working in the current multidisciplinary team. Exclusion criteria were the absence of professionals at the time of data collection, due to vacations and/or time off work, and being in the village at the time of data collection, since entry into indigenous territory was not allowed due to social isolation restrictions during the COVID-19 pandemic.
All the professionals in the nursing team were invited to take part in the study, and only one of them declined. Theoretical saturation of the data was reached by interviewing 12 professionals (six technicians and six nurses).
The participants were recruited through a nominal list, available and accessed on the website of the Caiuá Evangelical Mission - Mato Grosso do Sul Agreement, which is in the public domain.
Data was collected using an interview guide drawn up specifically for this research, validated by doctors with expertise in the subject or the technique adopted. A test interview was carried out, which did not need to be repeated and was included in the study.
The guide consisted of two distinctly categorized modules: the first related to sociodemographic issues such as age, gender, race/color, religion, and family income; as well as information related to characterizing the professional profile and professional qualifications of the interviewees, such as academic training, postgraduate studies/specialization. Data on training related to Indigenous health was also included, such as introductory training in Indigenous health, and training/courses already taken in indigenous health. Also in this module, data related to language barrier problems was collected: training for communication in the indigenous Guarani language; professional performance; number of villages and families served; total population served; daily commute to villages/workplace and means of transportation used.
The second module was made up of two generative questions: “Tell me a little about the beginning of your work in Indigenous health”. “Tell me about your day-to-day work, the demands imposed by working in an intercultural context, and how you care for indigenous alcohol users.”
The research was carried out between August and September 2021. The initial approach to the participants took place through two telephone contacts. The first contact was a presentation of the study's objectives and an informal invitation, and the second telephone contact was to schedule the date, time, and place for data collection, with priority given to taking place in their homes, on weekends and/or at times that would not compromise their work.
The interviews were carried out in the homes of the nursing professionals who made up the Indigenous health teams of two Indigenous Base Poles, located in two small municipalities in the south of the state of Mato Grosso do Sul. At the time of collection, only the participant and the researcher were present. All the professionals interviewed were working with the Guarani-Ñandeva and Kaiowá ethnic groups at the time of data collection.
The interviews lasted an average of 40 minutes. They were recorded on digital media and later transcribed in full. The researcher also used a field diary to record her perceptions and reflections. These records were later revisited, contributing to the triangulation of the data and aiding the process of understanding and analysis.
To process the data that refers to the characterization of the study participants (age, gender, race/color, religion, family income), an electronic spreadsheet of raw data was created using Microsoft Office Excel® 2019 software and analyzed using frequency and percentage to visualize the information of interest.
The narratives of the generative questions were analyzed under the methodological rigor of Content Analysis, defined as a set of communication analysis techniques aimed at describing the content of messages through a systematic and objective procedure.16
Based on the systematization of the Content Analysis procedure, through open and manual coding, the texts of the narratives were transformed into an organized and concise text of the main results evidenced in the analysis, identification of recurring terms, grouping of the units into larger categories and identification of the general theme. Triangulation of methods was used, combining interviews with field observations. To maintain the confidentiality of the research, each participant was represented by the letter P (Participants) followed by an alphanumeric number corresponding to the order in which the interview was inserted, for example, P1, and P2, among others.
From the textual corpus constituted from the participants' narratives, two thematic categories were identified: insertion into Indigenous health work and the cultural barriers to nursing care; Nursing work barriers to alcohol consumption in the intercultural environment of Indigenous care.
The study was conducted under national and international ethical guidelines and approved by the Research Ethics Committee (REC) of the State University of Paraná, with opinion no. 4.888.295/2021; CAAE: 50337021.1.0000.9247. In all the interviews, the Free and Informed Consent Term (FICT) was obtained from all the individuals involved in the study by signing it, after all questions had been read and clarified.
RESULTS
Twelve health professionals took part in the study, nurses and nursing technicians (6/6), aged between 33 and 57, the majority self-declared white race/color (10) and Catholic religion (nine), while three followed evangelical Christianity. Nurses earned an average of 7.66 minimum wages, while nursing technicians earned an average of three minimum wages, with two nursing technicians working double shifts.
The participants highlighted the challenges in nursing care related to qualifications, the language barrier, working conditions, cultural diversity, and alcohol consumption among the indigenous population (Chart 1).
Chart 1. Specific features of nursing care for the indigenous population. Iguatemi, (MS), Brazil, 2021.
|
Specifics |
Participants |
Notes |
|
Qualification and training |
Two nurses and four nursing technicians |
They have completed introductory training in Indigenous health: NIP* NTCP** ICPCD*** |
|
Adversities with the language barrier |
Three nurses; Six nursing technicians. |
They reported difficulty communicating in the Guarani language from the start of their working day. Of these, five claimed that this condition persisted. |
|
Condições de trabalho e questões da diversidade cultural |
Six nurses; six nursing technicians. |
All reported serving between one and five villages/camps, with the number of people and journeys varying: Families: between 250 and 900 family units; Population: <1000 to 5,946 people; Daily commute: Between 24 and 140 km. |
|
Alcohol abuse |
Two nurses; One nursing technician |
They were unaware of the reality of poverty, misery, and violence related to harmful alcohol consumption in Indigenous communities before they entered Indigenous health as professionals. |
*National Immunization Program; **National Tuberculosis Control Program; ***Integrated Care for Prevalent Childhood Diseases.
Regarding the training and qualification of professionals, the results of this study coincided with the period of the COVID-19 pandemic, when there was an intensification in the training of professionals working in indigenous health through digital platforms.
The language barrier was seen as a weakness in nursing care, especially among the elderly, as it hinders the interaction between the professional and the community. The professionals served varying numbers of families, in camps and villages with different population sizes, and traveled between 24 km and 140 km every day in the institution's cars to reach these areas.
Although a lack of knowledge about the indigenous reality was identified in this study, with only one professional claiming to have previous experience in this context, this topic was only explicitly mentioned by three nursing professionals.
Based on the textual corpus made up of the participants' narratives and to achieve the proposed objective employing Content Analysis, the results were structured into two categories: insertion into Indigenous health work and the cultural barriers to nursing care; nursing work barriers to alcohol consumption in the intercultural environment of Indigenous care.
Inclusion in Indigenous health work and cultural barriers to nursing care
Ten of the study participants began their professional careers in contact with Indigenous people in the locality of the study, and only two professionals had contact with other Indigenous communities.
The intercultural context, added to the milestones of the initial period of working with the Indigenous population, was pointed out by the participants as a challenging moment, identified through expressions such as: “I didn't understand”, “I didn't know”, “I had no idea of the reality of the Indigenous people” and “I thought about giving up”. In addition to these expressions, the lack of knowledge of the reality in the territories was also a factor that created obstacles to working.
When I entered indigenous health, it was very complicated, I didn't understand what it was, but after a while, I began to understand it [...]. (N1)
We know that it's differentiated health care, but I didn't know what this differentiated treatment was like, [...] the care itself doesn't differ, but inside (the village) you have to respect the culture [...]. (NT2)
When I joined in 2005 at the start of my career, [...] it was all very new, very different. I had no knowledge of it, I'd only heard about it. (N6)
There is a dichotomy in the participants' speeches about the concept of harmful and harmful use of alcohol in indigenous contexts, highlighting the stereotype of the “drunken Indian”, and associating cultural aspects with the consumption of industrialized drinks such as alcohol.
[...] being a resident of the municipality, I had some contact (with the indigenous people). At the time, I saw Indigenous people knocking on the door asking for food, drunk in the streets, [...] it wasn't scary to see Indigenous people, to have contact with them, they weren't different to me, but now you're acting as a professional...[...]. (N4)
[...] we understand that it's their culture, they prepare drinks with what they have there, which is cassava. So, on occasions of suffering, such as the departure of a loved one, they drink it, and it seems to forget a little about the pain and suffering they've experienced. Sometimes (they forget) even the misery, with alcohol. [...]. (NT6)
Nursing's labor barriers to alcohol consumption in the intercultural environment of Indigenous care
In order to meet the demands and develop care for Indigenous alcohol users, the nurses and nursing technicians highlighted prevention actions and individual guidance as the main intervention measures. These actions include talks at the BHU and schools, as well as referrals to psychologists.
“Lectures are given, and depending on the case, we refer people to the specific program in the municipality [...]. But the main thing we do here in the village are the talks, which are given by the nurses, doctors, and health workers”. (N6)
“Generally, when we detect that the patient needs help, we refer them to a psychologist, because there is a psychologist to carry out the assessment, and then pass them on to the responsible body, which is social assistance, to be monitored [...]”. (NT2)
“[...] Today we refer them to a psychologist. We receive him at the first moment, he goes for a consultation (at the BHU), the doctor asks for a quick test of everything and then we refer him to the psychologist”. (N2)
Nurses and technicians point out the specific programs for the management of cases of harmful use of alcohol that exist in the municipalities, but they show a lack of knowledge about how these programs work and highlight their inefficiency for the local indigenous context.
“[...] depending on that, we refer them to the specific program in the municipality. What's the name of the program? There's a specific program for this, you refer them to the municipality so they can offer other types of guidance [...].” (N6)
“[...] there's no program. A program was going to start in (the village), but it's very difficult for them to attend because they have to go every week [...]. The (last) time they went (to a service like this), it was in the municipality of Japorã”. (NT3)
The nursing professionals acted within the guidelines and goals established by the Ministry of Health for Primary Health Care (PHC), in implementing the actions of the programmatic areas. In the approach to Indigenous alcohol users, the actions did not overcome the barrier of moral/behavioral association for the harmful use of alcohol.
“It's a good job, you know, it's not bad, but there are times when you get discouraged [...] and I try to work towards targets, which is what I learned, preventive targets, vaccine targets”. (N1)
“We take care of the programs (programmatic actions), demand for vaccines, prenatal care, hyperdia [hypertension and diabetes] according to the schedule that the coordinator (technician) develops for us, preventive care, and other daily demands [...]”. (N5)
“[...] Let's start with screening for appointments, prenatal care, care for children, adolescents, the elderly, preventive care, administration of all vaccinations, [...] monitoring of tuberculosis, [...] notifiable diseases, nursing appointments [...]”. (N6)
“[...] when I see (the drunk Indigenous person) I tell them to go away, not to drink, but I say, if they listen to me, I don't know, so they leave [...]”. (N1)
The professionals who work directly with the indigenous population identify addictive behavior and the absence and/or inefficiency of intersectoral actions as the main challenges for nursing care for indigenous people in the context of the harmful use of alcohol.
[...] I had no idea what the reality of Indigenous people was like, it's a precarious situation [...] it was very impacting to see this reality (of drinking) [...]. I was shocked by the violence and alcohol consumption, even the fact that they wanted to attack us with words, [...] at first I thought several times about giving up working”. (N5)
[...] the situation of poverty and misery in the village is worrying. They're not committed to their work (alcohol users), but what's most worrying is self-aggression, aggression between themselves, between the family. They fight while drunk and mutilate themselves [...]. (NT6)
[...] unfortunately the only people in the village are the health services [...] and the school. The police don't come in very often, other programs that exist in the municipality don't happen in the village, he (the Indian) is always sought out to vote, they make everything easier, they put buses in [...], but resources for projects, it doesn't happen[...]. (N4)
DISCUSSION
The insertion of professionals in Indigenous villages is permeated with challenges and factors that trigger difficulties and multivariate dimensions of alcohol consumption in this population. Recognizing the cultural situation and using this information as a tool to predict actions and decisions for care in a congruent way is what supports the Theory of Diversity and Universality of Cultural Care14 and, in this way, the narratives presented describe the specificities of nursing care for the indigenous population of the Guarani-Ñandeva and Kaiowá ethnic groups with alcohol-related problems (Figure 1). It stands out from other national studies because it combines important elements such as the specific indigenous population, problematic alcohol consumption, and nursing professionals, during a pandemic period.17,18
The composition of nursing teams by gender in indigenous health follows the reality of the profession in Brazil, with a predominance of women. The age and length of service of the professionals are factors associated with the occurrence of emotional exhaustion, and doctors and nurses are more likely to have low personal fulfillment in indigenous health work than other professionals.19
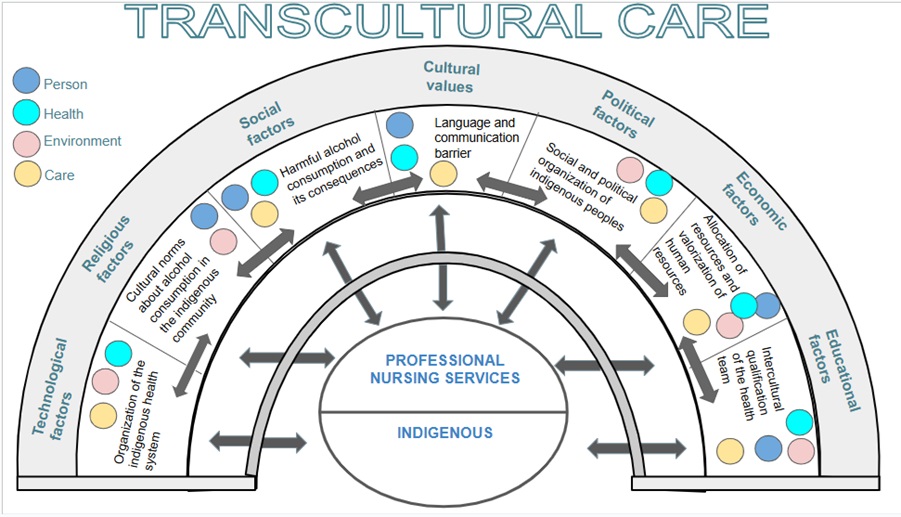
Figure 1. Cross cultural care. Iguatemi (MS), Brazil, 2024.
Source: Adapted from the Sunrise Model14 by the authors (2023).
Placing a worker in an intercultural context implies challenges and requires personal and interpersonal development supported by flexible professional education models.20 In Indigenous health, this transition is complex and affects both the professionals and the indigenous peoples. Thus, the qualification of professionals working in indigenous contexts must be constant, not limited to the beginning, but extending throughout the professional's career to develop cultural skills and critical thinking concerning the local health reality and the specific demands of this population.21
Qualified nursing work under appropriate working conditions plays an important role in maintaining the health and well-being of Indigenous communities since health is intrinsically related to the dimensions of life. In this way, the 2030 Agenda for Sustainable Development recognizes not only the collective rights of Indigenous people but also the active involvement and contribution of professionals who work with this population to achieve a safe and equal future, as outlined by the SDGs.22
Nursing professionals' statements about their lack of knowledge of the Indigenous reality at the beginning of their work, together with the identification of negative stereotypes, such as the “drunken Indian” and the association of the harmful use of alcohol with cultural aspects, highlight a significant problem in the training and practice of nursing in Indigenous contexts. This situation reflects both the lack of inclusion of specific content on Indigenous health in nursing training curricula and the presence of cultural prejudices that can negatively influence care for Indigenous populations.23,24
For the Guarani-Ñandeva and Kaiowá, alcohol use is deeply intertwined with historical issues of territorial loss, community disintegration, and socio-economic marginalization. The loss of traditional lands, which are fundamental to the identity and subsistence of these communities, contributes to feelings of hopelessness and cultural disintegration. This context of vulnerability intensifies alcohol consumption as a way of escaping from daily difficulties and historical suffering.25 Furthermore, in addition to the Guarani's own cultural practices, the introduction and availability of industrialized alcoholic beverages has exacerbated consumption, leading to harmful patterns of use that affect the physical, mental, and social health of these native peoples.26
In this sense, it is important to reflect on the health care implemented in the villages by the health teams, including the nursing team, through actions directed by the NPHCIP. IHCS works within the guidelines and targets set by the Ministry of Health, focusing on PHC. However, nursing professionals need to expand their work beyond the targets and guidelines, aiming for holistic care and applying critical thinking and decision-making based on their praxis in the Indigenous context. Otherwise, their actions will be conditioned to the size of the problem, which limits the effectiveness of their interventions.27
In the context of southern Mato Grosso, the Guarani-Ñandeva and Kaiowá ethnic groups, in addition to the problems caused by alcohol use, which is associated with historical and social factors such as the loss of traditional lands and the disintegration of community structures, face socio-economic marginalization, aggravated by the lack of public policies that are sensitive to their cultural specificities. In this sense, current interventions often fail by adopting a moralistic vision, without offering the support that respects and integrates the traditions of these ethnic groups.28
When approaching Indigenous alcohol users, nursing professionals do not overcome the barrier of moral and behavioral association concerning the harmful use of alcohol and Indigenous peoples. This means that, in many cases, actions are permeated by prejudice and moral judgment, rather than being based on a comprehensive and culturally sensitive understanding of the factors that contribute to alcohol use in these communities. These include prejudice, discrimination, and a lack of public policies. These policies should address socio-economic needs to strengthen existing protective factors within the organization of Indigenous society itself and reduce risk factors such as lack of income generation and poverty.29
Addictive behavior among Indigenous alcohol users makes it difficult to adhere to treatment. In addition, the lack of effective collaboration between different sectors, such as health, education, and social assistance, jeopardizes the implementation of integrated and comprehensive strategies. Intersectoral coordination is essential to address the social determinants of health and ensure that interventions are sustainable and effective in the long term. It is therefore essential to strengthen coordination between the different areas and promote collaborative work to improve the quality and effectiveness of the care provided to indigenous people.30
The fact that the study was aimed at nursing professionals with experience in Indigenous health care in two ethnic groups may be a limitation of the findings. This context points to the importance of future research with nursing professionals who provide care in different ethnic groups, and in other indigenous lands, where day-to-day care allows contact with indigenous people who abuse alcohol.
FINAL CONSIDERATIONS
Among the main obstacles faced by nursing professionals when dealing with harmful alcohol consumption among Indigenous people of the Guarani-Ñandeva and Kaiowa ethnic groups, as pointed out in this study, are a lack of knowledge of the Indigenous reality, a dichotomy concerning the concept of harmful and harmful alcohol use, reinforcing the stereotype of the “drunken Indian”.
Addictive behavior, often related to cultural aspects, reinforces a perspective among nursing professionals that therapeutic interventions are limited to this dimension. This view, when integrating cultural understanding with clinical practices, may inadvertently underestimate the multifaceted complexity of addiction, which includes biological, psychological, and social factors. Thus, by considering problems related to the harmful use of alcohol as a cultural issue, there is a risk of deviating from more holistic and integrated approaches, which are essential for effective and comprehensive treatment.
The absence or inefficiency of intersectoral actions emerges as one of the main challenges in nursing care for Indigenous people in the context of the harmful use of alcohol. This gap reveals a fragmented and uncoordinated approach, which compromises the effectiveness of interventions and perpetuates the vulnerability of this population. The lack of an integrated and collaborative response between the different health, social, and community sectors highlights the need for a critical reassessment of nursing practices, which are often passive in the face of this complex problem. It is therefore imperative that nursing professionals adopt a proactive and participatory stance, promoting intersectoral strategies that meet the specific needs of indigenous people, considering their socio-cultural reality and the multiple determinants of harmful alcohol use.
Nursing's holistic and integrated approach, focused on Indigenous people with problems resulting from the harmful use of alcohol, aims to overcome biomedical and fragmented actions in tackling this phenomenon. This approach, aligned with the SDGs, promotes more comprehensive and effective care, considering the multiple determinants of health and respecting the socio-cultural complexity of the Indigenous population.
CONTRIBUTIONS
Daniela Aparecida de Souza Nunes: conception and planning of the study, data collection, analysis and interpretation; drafting and/or critical revision of the manuscript; Adriana Martins Gallo: drafting and/or critical revision of the manuscript; Francielle Renata Danielli Martins Marques: drafting and/or critical revision of the manuscript; Giovana Alves Santos: drafting and/or critical revision of the manuscript; Lashayane Eohanne Dias: drafting and/or critical revision of the manuscript; Maria Aparecida Salci: drafting and/or critical revision of the manuscript; Lígia Carreira: conception and planning of the study, data collection, analysis and interpretation; drafting and/or critical revision of the manuscript.
CONFLICT OF INTEREST
Nothing to report.
REFERENCES
- Instituto Brasileiro de Geografia e Estatística. Dados do censo de 2022 revelam que o Brasil tem 1,7 milhão de indígenas. 2022. Available from: https://www.gov.br/funai/pt-br/assuntos/noticias/2023/dados-do-censo-2022-revelam-que-o-brasil-tem-1-7-milhao-de-indigenas
- Carvalho EMC, Santos RL. Literatura Indígena: Entre Memórias. Educação em Revista. 2023:1-12. DOI: http://dx.doi.org/10.1590/0102-469838419
- Cisa - Centro de Informações sobre Saúde e Álcool. Álcool e a Saúde dos Brasileiros: Panorama. 2023, 1. ed. - São Paulo, SP. Available from: https://cisa.org.br/images/upload/Panorama_Alcool_Saude_CISA2023.pdf
- Assunção AKM, Branco MRFC, Santos TS, Costa SSB, Júnior JJD, Frota MTBA, Oliveira BLCA. Comparação dos casos de beribéri entre indígenas e não indígenas, Brasil, 2013 a 2018. Ciênc. saúde coletiva [Internet]. 2023 [cited 2023 Nov 2];28(7). DOI: https://doi.org/10.1590/1413-81232023287.16422022
- Castelo-Branco FMF, Vargas D. Binge drinking e fatores associados em indígenas da etnia Karipuna. Rev. Eletrônica Saúde Mental Álcool Drog [Internet]. 2021 [cited 2023 Nov 28];17(1):7-16. DOI: https://dx.doi.org/10.11606/issn.1806-6976.smad.2021.167996
- Cavicchioli MR. La botte piena o la moglie ubriaca? Vinho e gênero na Roma antiga. Rev. Archai. 2023;33:e033009. DOI: https://doi.org/10.14195/1984-249X_33_09
- Souza RSB de, Oliveira JC de, Teodoro MLM. Construction of an Instrument to Evaluate the Use of Alcoholic Beverages in an Indigenous Ethnic Group of Minas Gerais. Psicol ciênc prof [Internet]. 2019;e176628(39):1-11. DOI: https://doi.org/10.1590/1982-3703003176628
- Barreto IF, Dimeinstein MDB, Leite JF. Percepções sobre o uso de álcool em uma comunidade indígena potiguár. Psicologia: Teoria e Pesquisa. 2022;e38419(38):1-10. DOI: https://doi.org/10.1590/0102.3772e38419.pt
- Wayhs ACD, Bento BAR, Quadros FAA. Public policies on indigenous mental health in Brazil. Trayectorias Humanas Trascontinentales. 2019;(4) DOI: https://doi.org/10.25965/trahs.1577
- Miranda WD, Silva GDM, Fernandes LMM, Silveira F, Sousa RP. Desigualdades de saúde no Brasil: proposta de priorização para alcance dos Objetivos do Desenvolvimento Sustentável. Cad. Saúde Pública. 2023;(39):e00119022. DOI: https://doi.org/10.1590/0102-311XPT119022
- Monteiro MAC, Siqueira LEA, Frota NM, Barros LM, Holanda VMS. Assistência de enfermagem à saúde das populações indígenas: revisão de escopo. Cogitare Enfermagem [Internet]. 2023 [cited 2023 Nov 2];28. DOI: https://doi.org/10.1590/ce.v28i0.91074
- Silva MD, Rodriguez AR, Silva CRS, Farias ECMH, Nascimento JA, Lima MM, Seffair RP, Dourado TC. Narrative study on the health of the elderly in the indigenous area. Brazilian Journal of Development [Internet]. 2021 [cited 2023 Nov 2];7(8). DOI: https://doi.org/10.34117/bjdv7n8-506
- Minayo MCS. Origem inusitada da pesquisa qualitativa em ciências sociais no Brasil. Hist. Ciênc. Saúde-Manguinhos. 2020;27:919-32. DOI: https://doi.org/10.1590/S0104-59702020000400012
- Leininger MM. Transcultural care diversity and universality: a theory of nursing. Nurs Health Care. 1985;6(4):208-12. Available from: https://pubmed.ncbi.nlm.nih.gov/3846132/
- Dahlstrom MF. The narrative truth about scientific misinformation. Proceedings of the National Academy of Sciences of the United States of America. 2021;118(15). DOI: https://doi.org/10.1073/pnas.1914085117
- Bardin L. Análise de Conteúdo. Tradução: Luís Augusto Pinheiro. 2016;70:141. Available from: https://madmunifacs.files.wordpress.com/2016/08/anc3a1lise-de-contec3bado-laurence-bardin.pdf
- Freitas MG, Stopa SR, Silva EN. Consumo de bebidas alcoólicas no Brasil: estimativa de razões de prevalências – 2013 e 2019. Revista de Saúde Pública [s. l.]. 2023. DOI: https://doi.org/10.11606/s1518-8787.2023057004380
- Cisa – Centro de Informação sobre saúde e álcool. Álcool e a saúde dos brasileiros: Panorama 2021. São Paulo: Cisa, 2021. Available from: https://cisa.org.br/images/upload/Panorama_Alcool_Saude_CISA2021.pdf
- Ferraz JAC, Zanin L, Gomes AM, Flório FM. Prevalência e fatores associados à síndrome de burnout em profissionais da saúde indígena no Brasil. Ciência & Saúde Coletiva, 2023;28(1):93-106. DOI: https://doi.org/10.1590/1413-81232023281.09272022
- Dzidowska M, Lee KSK, Conigrave JH, Dobbins TA, Hummerston B, Wilson S, Haber PS, Gray D, Conigrave KM. Apoio aos serviços de saúde aborígenes na redução dos danos causados pelo álcool: resultados da prestação de serviços de 2 anos num ensaio randomizado de agrupamento. Wiley online library [Internet]. 2021 [cited 2023 Nov 2];117(3):796-803. DOI : https://doi.org/10.1111/add.15712
- Chen F, Liu Y, Wang X, Dong H. Transition shock, preceptor support and nursing competency among newly graduated registered nurses: A cross-sectional study. Nurse Educ Today [Internet]. 2021;102:104891. DOI: https://doi.org/10.1016/j.nedt.2021.104891
- Zeifert APB, Censi DR, Manchini A. A justiça social e a agenda 2030: políticas de desenvolvimento para a construção de sociedades justas e inclusivas. Direitos Sociais e políticas públicas (UNIFAFIBE) [Internet]. 2020 [cited 2023 Nov 2];8(2):30–52. Available from: https://portal.unifafibe.com.br/revista/index.php/direitos-sociais-politicas-pub/article/view/766
- Maia AS, Nascimento EM do, Carvalho TP de, Sousa CG de. Os desafios da enfermagem na atenção integral a saúde dos povos indígenas. Enferm em Foco. 2021;12(2):333–8. DOI: https://doi.org/10.21675/2357-707X.2021.v12.n2.4166
- Santos J, Carmo CN, Características da violência por parceiro íntimo em Mato Grosso do Sul, 2009-2018. Epidemiologia e Serviços de Saúde, Brasília. 2023;32(1):e2022307. DOI: https://doi.org/10.1590/S2237-96222023000100019
- Paredes YV, Yarce E, Aguirre DC. Condiciones sociodemográficas y perfil de salud de los adultos mayores indígenas del departamento de Nariño. Rev. Cienc. Salud. 2019;18(1)67-81. DOI: https://doi.org/10.12804/revistas.urosario.edu.co/revsalud/a.8764
- Oliveira RC, Nicolau BF, Levine A, Mendonça AVM, Videira V, Vargas AMD, et al. “When a tihik drinks kaxmuk he neither has a father, nor a mother, or a brother”: Perceptions of maxakali on the effects of sugarcane liquor consumption. Cienc e Saude Coletiva. 2019;24(8):2883–94. DOI: https://doi.org/10.1590/1413-81232018248.16992017
- Rodrigues RP, Barroso RF, Emmi DT, Santos JG. Análise das ações e serviços voltados à saúde indígena nos planos regionais de redes de atenção à saúde do Pará. Saúde em Redes. 2021;6(3):13–23. DOI: https://doi.org/10.18310/2446-4813.2020v6n3p13-23
- Pontes AL, Machado FRS, Santos RV, Brito CAG. Diálogos entre indigenismo e Reforma Sanitária: bases discursivas da criação do subsistema de saúde indígena. Saúde Debate. 2019;43. DOI: https://doi.org/10.1590/0103-11042019S811
- Amorim TS, Backes MTS, Carvalho KM, Santos EKA, Dorosz, PA, Backes DS. Gestão do Cuidado de Enfermagem para a qualidade da assistência pré-natal na Atenção Primária à Saúde. Esc Anna Nery. 2022;26:e20210300. DOI: https://doi.org/10.1590/2177-9465-EAN-2021-0300
- Hitchon CA, ONeil L, Peschken CA, Robinson DB, Fowler-Woods A, El-Gabalawy HS. Disparities in rheumatoid arthritis outcomes for North American Indigenous populations, International Journal of Circumpolar Health. 2023;82(1):2166447. DOI: https://doi.org/10.1080/22423982.2023.2166447
Correspondence
Daniela Aparecida de Souza Nunes
E-mail: danisouza.enf@gmail.com
Copyright© 2024 UFPE Nursing Journal online/REUOL.
This is an open-access article distributed under the CC BY 4.0 Creative Commons Attribution-ShareAlike 4.0 International License, which allows others to distribute, remix, adapt, and create from your work, even for commercial purposes, as long as they credit you for the original creation. It is recommended to maximize the dissemination and use of licensed materials.
 Português (Brasil)
Português (Brasil)  English
English  Español (España)
Español (España) 



















