
Idioma
PNAB y la promoción de la salud en el SUS: contribuciones de las producciones académicas de programas de posgrado en salud en el norte/noreste de Brasil
![]() Luciana Dantas Farias de Andrade1,
Luciana Dantas Farias de Andrade1, ![]() Stephany Raquel Leonço Mota2,
Stephany Raquel Leonço Mota2, ![]() Crisalda Eslita Silva Silveira3,
Crisalda Eslita Silva Silveira3, ![]() Marcela Samara Lira da Silva4,
Marcela Samara Lira da Silva4, ![]() Maria Clara Soares Dantas5
Maria Clara Soares Dantas5
1,2Universidade Federal da Paraíba. João Pessoa (PB), Brazil. 3Universidade Federal de Campina Grande. Campina Grande (PB), Brazil. 4Universidade Federal do Rio Grande do Norte. Caicó (RN), Brazil. 5Escola de Enfermagem Ana Nery. Cidade Nova (RJ), Brazil.
Introduction
The Brazilian Unified Health System (SUS), formalized by Law No. 8,080/90, is Brazil's main public health policy, understood as an integrated set of actions and services at the care and administrative levels provided by the government1. Also known as the Organic Health Law, it establishes health as a fundamental right of all citizens, assigning the State the responsibility of implementing policies for the promotion, prevention, and recovery of the health of the population it serves2.
The organizational principles of universality and comprehensiveness of healthcare provided by the SUS underpin the provision of services to all Brazilian citizens, without cultural, geographical, social, or social vulnerability distinctions3, meeting health requirements ranging from Primary Health Care (PHC) to highly complex services4. In this context, the Family Health Program (FHP) emerged in 1994 as a model of care developed to shift the matrix of Primary Health Care from a model centered on the treatment of diseases to a biopsychosocial health model focused on the real needs of SUS users5-6.
Considered synonymous with APS, Primary Health Care (PHC) is defined as a set of individual and collective actions aimed at health promotion, treatment, diagnosis, disease prevention, harm reduction, and health maintenance, with the aim of strengthening the comprehensiveness of the health system7. In line with this proposal, in 2006, the first edition of the National Primary Care Policy (PNAB) was published, establishing itself as one of the essential pillars for the organization of primary care in Brazil. This policy recognizes Family Health as a model for reorganizing care, addressing infrastructure, resources, and team organization, with a focus on health promotion, disease prevention, and the provision of continuous health care to the population8.
PHC is an essential component of health systems in many countries, not just Brazil. In the United Kingdom, the Dawson Report of 1920 emerges to advocate for the organization of health services, characterized by the hierarchization of levels of care and the strengthening of relationships between curative and preventive actions, seeking to promote health to most of the British population9.
In this sense, different countries around the world have different PHC organizations, incorporating aspects of the British National Health System and the 1978 Alma-Ata Declaration, signed by the member countries of the World Health Organization (WHO) as a pact that proposed the establishment of local health services based on an interdisciplinary perspective and focused on the needs of the population, a fundamental reference for the reforms that have taken place in the health systems of various countries around the world since the 1980s and 1990s10.
In subsequent decades, the redemocratization of Latin American governments and their commitment to social justice reaffirmed the principles established in Alma-Ata through the revitalization of PHC. In Brazil, these principles were reflected in the structuring of the SUS, a model of care that emphasizes social inclusion, equity, and comprehensive care, highlighting its importance as a universal health system of quality, efficiency, and equity in care, with an emphasis on the organization of comprehensive PHC, public financing, and effective state regulation to guarantee universal access, viewing health as a public good11.
In Bolivia, the set of reforms implemented in the 1990s culminated in the consolidation of the Intercultural Community Family Health Policy (SAFCI, in Portuguese), conceived as a PHC strategy based on the principles of community participation, intersectorality, interculturality, and comprehensiveness. In this context, the intercultural approach is particularly advanced, as interculturality is a pillar of national health policy, as evidenced by the systematic coordination between PHC teams and traditional healers within their respective areas of responsibility to integrate biomedical knowledge and ancestral practices into care processes12-13. As observed in the experiences of Bolivia and Brazil, social participation in the formulation and execution of health actions and services is a central element in ensuring the sector's responsiveness to the needs of the population, as well as in strengthening democracy and guaranteeing social rights14.
Thus, postgraduate courses in Public Health or Family Health play a crucial role in training and qualifying specialized professionals to work in PHC. In this context, in addition to generating scientific knowledge, the academic output of these programs serves as a strategic tool for the development of health practices in PHC. Due to their construction based on rigorous methodologies and guided by concrete problems in the daily routine of health services, such productions enable the identification of local needs, the organization of work processes, the evaluation of new approaches, and the proposal of innovative solutions to the challenges of each region15, driving the continuous improvement of the quality of care offered to the population.
Furthermore, the study is justified by the centrality of the PNAB in the organization of PHC in the SUS and by the need to evaluate its contributions to the strategic axis of Health Promotion. It should be noted, then, that the analysis of academic production is a robust method for mapping the knowledge generated in graduate programs operating at the forefront of the system, especially in the North and Northeast of Brazil, regions whose experiences and challenges are crucial for improving health policies.
Given the relevance of PHC as a strategy for implementing the organizational principles of the SUS in Brazilian healthcare, playing a crucial role in disease prevention and health promotion, the objective was to analyze the contributions of the PNAB to the effectiveness of health promotion in the SUS, based on academic publications from postgraduate programs in Family Health and Public Health in the North and Northeast regions of Brazil.
Method
This is a documentary study with a qualitative approach, using textual materials from dissertation and thesis abstracts collected between February and March 2025 from the repositories of the Postgraduate Courses in Public Health and Family Health offered at the most essential Federal Universities in the North and Northeast states of Brazil.
The inclusion criteria for document selection included academic publications from 2020 to 2024, limited to works available in the institutional repositories of Federal Universities in the North and Northeast regions of Brazil. Exclusion criteria included studies that were not fully available in the repositories cited. The sampling criterion was defined based on the availability of collections, using all dissertations and theses defended in the Family Health and Collective Health Graduate Programs in the North and Northeast that were made available in repositories between 2020 and 2024.
The application of a structured data collection protocol proved fundamental to ensuring the standardization, reliability, and traceability of information compiled from the transcription of the abstracts of theses and dissertations linked to the Graduate Programs in Public Health and Family Health in the North and Northeast regions. The protocol covered institutional and geographic variables, such as the graduate program of origin, the North or Northeast region of the country, the state, and the university where the work was produced, and the number of theses defended between 2020 and 2024 at those institutions.
In addition, essential information for the individual characterization of each production was incorporated into the protocol, including the nature of the work, which may be a thesis or dissertation, the title, and the publication date. This systematization enabled careful organization of the document corpus, ensuring uniformity in data extraction and enabling comparative analyses across institutional and regional contexts.
It should also be noted that, as these documents are publicly accessible, the study is exempt from the consent requirement under the General Data Protection Law, thereby emphasizing respect for copyright and the citation of sources16. The textual material found was organized and categorized using Iramuteq software.
Content Analysis, chosen for analyzing empirical material, seeks to uncover hidden meanings, examines the significance of words, and systematically establishes correlations between linguistic and social structures that can describe the characteristics of language and social groups17.
As Bardin advises, Content Analysis is structured in three distinct stages: pre-analysis, exploration of the material, and treatment of the results18. Pre-analysis, the first organizational stage, consists of conducting a preliminary analysis of the data, through phases of floating reading, organization of the material, with the selection of documents and definition of objectives, referencing of indexes, and the development of hypotheses and indicators. Consequently, the material exploration stage entails a thorough analysis of the content, in which raw data are transformed into categorical representations of the corpus. Finally, the stage of analysis and processing of results is conducted through inference and logical interpretation of the content identified in the texts19.
In the first stage of Content Analysis, pre-analysis, there was a preliminary analysis of the abstracts of master's dissertations and doctoral theses of graduate students in Public Health and Family Health, which were gathered into a single corpus, allowing initial contact with the materials through skimming, seeking to understand the collected texts, and delimiting the analysis and objectives of the research.
The second stage, the exploration of the material, took place after the organization and submission of the corpus for categorization using the Iramuteq software, resulting in the distribution of text segments, by statistical relevance, in a Descending Hierarchical Classification (DHC)20, categorizing the words according to their similarities and thus creating five different classes, named based on the PNAB and its applications in the provision of health services and in postgraduate academic and scientific studies.
The third stage, analysis and treatment of results, was conducted in accordance with the epistemological assumptions of content analysis. By analyzing the classes generated by the software, it was possible to develop the following thematic categories: class 3 gave rise to thematic category 1: Universality in Primary Care; the combination of classes 1 and 2, which converged in the dendrogram, gave rise to thematic category 2: Primary Health Care: Multiple professional approach to health promotion and disease prevention;; from class 4, thematic category 3 originated: Primary Care in times of Covid-19; thematic category 4 originated from class 5: Scientific Approaches in the Study of Collective Health.
Results
For the analysis, 353 documents were selected, of which 290 were master's theses, and 63 were doctoral dissertations. Using the Descending Hierarchical Classification (DHC) method, 3,400 text segments were selected; 3,178 were retained, representing 93.47% of the total, exceeding the recommended minimum of 70% for data utilization21. In this analysis, the Iramuteq software grouped the words into five different lexical classes (Figure 1), named based on the interpretation of the grouped terms and the thematic focus of the research, to understand the meanings attributed to each word in the categories generated by the software.
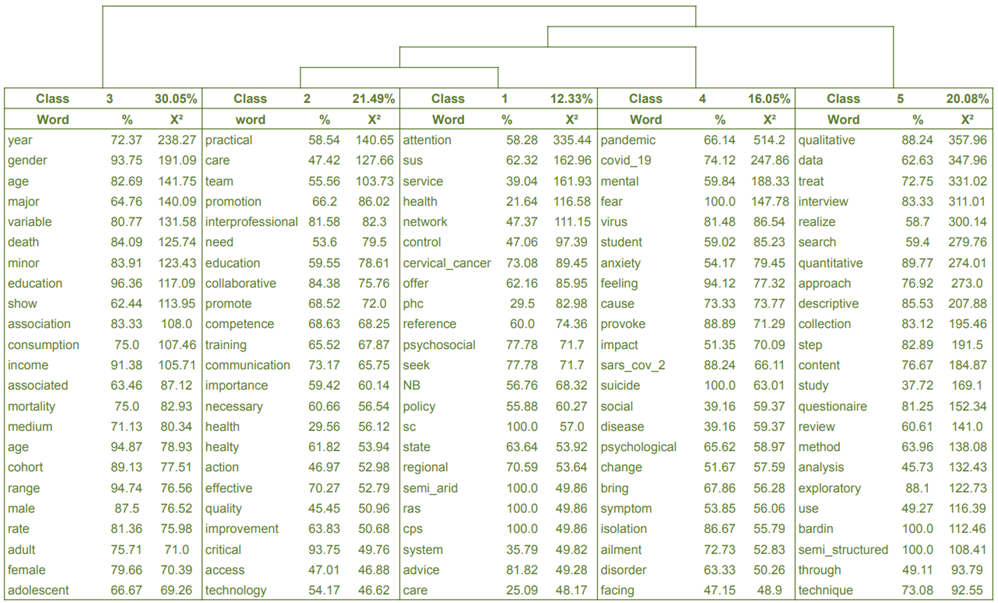
Figure 1- Dendrogram of the corpus of abstracts from the abstracts produced in the Postgraduate courses in Public Health and Family Health. João Pessoa (PB), Brazil, 2025.
The dendrogram (Figure 1) shows the result of processing the textual corpus, identifying five semantic classes originating from that corpus, namely: Class 1, with 392 text segments, corresponding to 12.33%; Class 2, with 683 segments, representing 21.49%; Class 3, with 955 text segments, corresponding to 30.05%; Class 4, with 510 text segments (16.05%); and Class 5, with 638 text segments, representing 20.08% of the 3,178 text segments used.
About the classes derived from the analyzed corpus, illustrated in Figure 1, it is possible to observe two branches, one covering only class 3 and the other comprising the remaining classes. In the first subdivision, class 5 is isolated, while the subsequent subdivision branches off with another solitary class, class 4, covering classes 1 and 2 in the same branch.
Considering that the contextual affinity between classes is illustrated by their proximity, there is a greater affinity between the texts found in classes 1 and 2, which, in turn, are distant from the other classes, containing words related to the organization and functioning of PHC in the context of the SUS. Class 5, with words strongly associated with ‘qualitative’ ‘data’, and ‘interview’, shows that most of the academic production analyzed uses a qualitative approach, thereby validating the corpus constructed for the proposed analysis.
The Chi-square test (χ2), which indicates the associative strength between words and their respective classes22, pointed to a higher degree of statistical significance for the words in class 5, demonstrating its prevalence among the other classes, with its words related to the methods used in the construction of the academic productions used. Using Iramuteq, it is possible to verify that class 5 is characterized by the words: qualitative (χ2 = 357.96), data (χ2 = 347.96), treat (χ2 = 331.02), interview (χ2 = 311.01).
Discussion
Universality in Primary Care
Originating from class 3, thematic category 1 represents 30.05% of the text segments, considered the most representative among the classes, and has as its main words: age, education, income, mortality, and gender. As one of the doctrinal principles of the SUS, universality, expressed by the words gathered in this category, is expressed in primary care through the reception without exclusionary differentiations of individuals who seek health services, considering the determinants and conditions of health, and offering health care adapted to the needs of individuals in their multiple realities23.
PHC acts as the gateway to the SUS, being the sector responsible for building a positive link between the health service and the community, thus facilitating the continuity of quality care and resolvability24.
In this context, PHC has a significant impact on health analysis indicators, with particular emphasis on its contribution to reducing infant mortality, which became more evident after the implementation of the PNAB in 2006. Among other measures, this program expanded basic healthcare to a larger portion of the Brazilian population, with the increase in the monitoring of pregnant women and the increase in vaccination coverage as determining factors for the reduction of these indicators25.
The role of Community Health Workers (CHWs) in maternal and child health care is a strategic component of PHC. CHWs perform fundamental functions in the comprehensive care of pregnant women and children across different stages of development, conducting home visits to monitor growth, development, and health, and providing guidance on childcare consultations and immunization administration at appropriate times. Thus, the work of CHWs is essential to strengthening continuous, comprehensive, and community-based care, thereby promoting maternal and child health26.
Between 2000 and 2015, the infant mortality rate (IMR) in Brazil fell by 45.07%. Studies indicate that the IMR is directly associated with the infrastructure of Basic Health Units (BHUs), suggesting that more structured services improve access and the adequate monitoring of severe cases, thereby reducing income-related health inequalities. Despite these advances, significant geographical disparities persist, especially in the North and Northeast regions, where municipalities further away from the capitals recorded a smaller reduction in the IMR, and even areas close to the capitals of the North presented unsatisfactory results, reinforcing the need to expand and strengthen Family Health Teams (FHT) as a central instrument in promoting equity and improving child health27.
Furthermore, CHWs play an essential role in combating vaccine-preventable diseases and expanding vaccination coverage, as their duties include disease prevention and health promotion activities conducted in the home or community, both individually and collectively, in accordance with guidelines established by SUS28. Their direct and continuous contact with families, combined with their knowledge of local living conditions and vulnerabilities, strengthens the relationship of trust between the population and health services, encouraging adherence to immunization actions and contributing to reducing vaccine hesitancy29.
The effectiveness of PHC in monitoring historically vulnerable population groups, such as homeless people, indigenous communities, and populations in rural areas30, is also evidenced, being a crucial sector for ensuring access to health care without discrimination based on geographic origin, social class, gender, and age.
PHC is the main gateway for homeless people, using specific strategies, such as the Street Clinic, to reduce bureaucratic and sociocultural barriers. Despite its central role in access, difficulties persist in establishing links and continuity of care, given the multiple vulnerabilities that characterize this group. Thus, the implementation of comprehensive and multidisciplinary care, linked to intersectoral policies and the training of teams, is essential for PHC to respond more adequately, equitably, and effectively to the complex needs of homeless people31.
In the context of indigenous communities, PHC plays a central role in ensuring universal care by incorporating the cultural, territorial, and epidemiological characteristics of these peoples. The Indigenous Health Care Subsystem (SASI), designed to organize PHC in indigenous territories and ensure continuity of care at different levels of care, embodies this purpose by recognizing and integrating traditional knowledge, ensuring participation and social control, and adapting care practices to local sociocultural specificities. Consequently, the development of the National Policy for Indigenous Peoples' Health Care is a concrete expression of the effort to bring together teams that combine traditional knowledge with biomedical practices32.
A study conducted at the Alto Rio Negro DSEI in the state of Amazonas evaluated the attributes of PHC from the perspective of professionals and found that difficult physical access and cultural barriers require specific adaptations, such as the existence of base centers, receiving patients referred by indigenous health agents and, when necessary, referring them to higher levels of care in municipal centers33. In addition, the recent implementation of SASI hubs in northeastern states, such as Rio Grande do Norte and Piauí, demonstrates the institutional effort to expand the indigenous health network in these regions, promoting more equitable and geographically accessible primary care.
In remote rural areas, PHC is also crucial to realizing the principle of universality, addressing structural geographic inequalities. A study conducted in remote rural municipalities in western Pará documented how socioeconomic conditions, climate, and difficulties in retaining professionals limit service coverage, while mobile services, expanding the tasks of community agents, and support from family health teams are essential to maintaining access and comprehensive care34.
A field study conducted in the municipality of Assis Brasil, Acre, home to riverside and indigenous communities such as the Jaminawa and Manchineri peoples, showed that despite significant challenges in terms of infrastructure, staff shortages, and logistics, the UBS are central elements of primary care, treating conditions such as hypertension, prenatal care, and cancer. The FHSs and, especially, the CHWs play a fundamental role in promoting local health, guiding sanitation, nutrition, and physical activity, and identifying users and areas with the greatest need for follow-up, highlighting the importance of PHC as a means of realizing the right to health for marginalized rural populations35.
Primary Health Care: health promotion and disease prevention
Representing 33.82% of the text segments, thematic category 2, originating from classes 1 and 2, has the following main emblematic words: team, interprofessional, competence, training, communication, care, SUS, cervical cancer, psychosocial, and care.
As the gateway to health services, PHC provides guidelines for individual or collective health actions through a multidisciplinary team focused on the needs of the community in which it operates, guiding the formation of health teams that promote collaboration between doctors, nurses, dentists, pharmacists, and other professionals, while respecting the competencies and specificities of each area36. In this way, PHC aims to integrate knowledge and practices from different areas of expertise, enhancing the effectiveness and continuity of care, in addition to ensuring more comprehensive care focused on the needs of the user.
To ensure the effectiveness of the services provided by PHC, it is necessary for the health team to be prepared to work in a collaborative and integrated manner. In accordance with the latest version of the PNAB, continuing education gains relevance for its contribution to the adoption of tools to improve health actions and services and to the feasibility of expanding the critical capacity of professionals, considering professionals' experiences in the service context during their training37.
Even facing the absence of formal training, teams play a leading role in the autonomous search for knowledge, underscoring the need for continuous, contextualized training processes. Experiences such as the Education through Work for Health Program (PET-Saúde) demonstrate that integration between educational institutions, services, and communities favors critical training and the development of shared solutions to territorial challenges. Thus, continuing education establishes itself as a tool for ensuring the quality of health services, as it guarantees that PHC offers adequate, accessible care focused on the needs of users, promoting equity and efficiency in the SUS38.
As one of the fundamental pillars of the SUS, the PNAB aims to organize the healthcare network in a comprehensive manner, which is a crucial aspect in the implementation of strategies for the prevention of highly relevant public health problems, such as noncommunicable diseases (NCDs), with an emphasis on the prevention and screening of cervical neoplasms39. In this context, cytopathological examination (Pap smear) stands out as the primary tool for screening cervical cancer, offered to women between 25 and 64 years of age on an annual basis40, and is a technically legitimate intervention scientifically proven to be effective in reducing the incidence and mortality rates of cervical cancer41.
The organization of health services and the actions of professionals, as well as the education, income, and moral values of health system users, are significant aspects for the perception of preventive practices and the achievement of satisfactory results. Barriers such as difficulties in accessing health facilities, poor customer service, lack of guidance on cervical cancer prevention, limitations in infrastructure and scheduling of exams, delays in delivering results, and difficulty in accessing specialized services are associated with not performing Pap smears. All these aspects require improvements in the planning of actions for cervical cancer prevention in the North region of Brazil, which is the region with the highest mortality rate between 2011 and 202142-43.
The study shows a temporal trend characterized by an increase in cervical cancer mortality rates in Brazil between 2015 and 2018, followed by a reduction in the period from 2018 to 2021. At the same time, between 2020 and 2021, there was a significant increase in cytopathological examinations among women aged 24 to 64 within the SUS, the priority age group for screening. The expansion of this coverage, which is essential for early detection of precursor lesions, may have contributed to the decline in mortality observed after 2018 by promoting timely diagnoses and more effective interventions in disease management44.
A study conducted in Manaus, Amazonas, showed that reorganizing the workflow, implementing a new service flowchart, and expanding the availability of cytopathological tests were decisive factors in strengthening the bond between the health team and users, with a 36% increase in collections compared to the previous year. In this sense, through the FHS, PHC can and should play a central role in strengthening health promotion activities through educational strategies grounded in dialogue, welcome, and empathy, thereby favoring female leadership in self-care and cervical cancer prevention45.
Furthermore, prevention against Human Papillomavirus (HPV) is essential to improve the prognosis of women already diagnosed and to reduce the incidence of cervical carcinoma, since it is the microorganism responsible for the development of most cases. Since 2014, the HPV vaccination campaign for children aged 9-14 years has been established as an effective PHC strategy to protect against the most common oncogenic HPV types and prevent precancerous lesions46.
Despite the efforts of the APS, HPV vaccination coverage in Brazil is on a downward trend, with the first dose administered to 87.08% of girls aged 9 to 14 in 2019, falling to 75.81% in 2022, and among boys, from 61.55% to 52.16% in the same period, levels that are insufficient to optimize the prevention of the virus and cancer precursor lesions. Achieving coverage rates close to 90% could significantly reduce the incidence of HPV and its complications. Thus, vaccine adherence is a central strategy in cancer prevention, requiring educational campaigns, greater engagement by schools, and actions to combat misinformation to ensure positive impacts on public health47.
Furthermore, the abstracts analyzed show that PHC also demonstrates its interprofessionality through the Family Health Support Centers (NASF, in Portuguese), created in 2017 as a set of multidisciplinary teams that should work in an integrated manner with the Family Health Teams, basing their actions on matrix support and interprofessional work, with a view to integrating care and the resolvability of actions within the scope of the FHS48.
An analysis of data from Cycles II and III of the National Program for Improving Access and Quality of Primary Care in three Northeastern states revealed the broad scope of NASF teams in mental health care. In Cycle II, 84.6% of teams provided care to people with psychological distress and/or mental disorders, 88% offered joint follow-up with Primary Health Care (PHC), and 91% conducted home visits. In Cycle III, 94.7% of teams developed mental health actions, 80.9% monitored cases in partnership with CAPS, reaching 88.9% in municipalities with traditional populations, and 91.3% supported cases of psychoactive substance use, reaching 96.8% in the most vulnerable territories. These results highlight the essential role of NASF in expanding access, improving shared care, and coordinating the psychosocial care network in contexts marked by social vulnerability49.
In 2023, NASF/AB was replaced by the Multidisciplinary Primary Care Team (eMulti), emerging as an alternative to the previous model. To broaden the scope of practices and resolvability in PHC, eMulti seeks to facilitate the population's access to health care and integrate aspects of care, prevention, promotion, surveillance, and health training, expanding the diversity of professionals who can compose PHC care teams50.
Therefore, through the integration of basic and specialized care, PHC plays an important role not only in reducing the incidence and mortality of oncological diseases, but also in the prevention and monitoring of psychological disorders, as it offers care that extends to the community, facilitating adherence to treatment and ensuring continuity of care.
Primary Care in Times of COVID-19
Thematic category 3 (16.05%) includes the following words relevant to knowledge construction: pandemic, COVID-19, impact, fear, psychological, and disorder. The pandemic caused by the SARS-CoV-2 virus, due to its rapid transmission across continents, has had a direct effect on the mental health of the population, including health professionals and users of health services. The reorganization of PHC was essential to tackle the COVID-19 pandemic, with the need to adapt the protocols and guidelines defined by the Ministry of Health (MH) and WHO to the reality of each region51.
Despite this, studies indicate a lack of leadership by the Brazilian Ministry of Health, which, in the face of one of the most significant health events in the SUS's history, did not issue guidance on the development of actions by PHC multidisciplinary teams. In this context, as the Recife Health Department's recommendations demonstrate, protocols for the healthcare and clinical management of COVID-19 were left to state governments, making it difficult to anticipate potential changes to PHC activities facing the health crisis52-53.
Even in this context, the bond, and proximity of professionals with the population and their knowledge of the territory were crucial characteristics that enabled PHC actions in monitoring suspected and mild cases, with PHC being the foundation for the response in emergencies and a strong ally for the implementation of the necessary care to combat COVID-19 in Brazil54. Thus, PHC stood out for its strategic collaboration in reducing the risk of disease transmission, anchored in early diagnosis, individual and collective care of individuals, as well as being the front line in ensuring access to vaccination for the Brazilian population55.
It is essential, then, to consider the central importance of PHC during the pandemic in northeastern Brazil, which had a 6% higher prevalence of referrals of users at risk of worsening COVID-19 to other points of care in the Health Care Network than the North and South regions. This can be explained by the greater coverage of the ESF in this region, indicating that more teams and health professionals provide continuous monitoring of health system users. Thus, it is possible to understand that rigorous monitoring and training of health teams were essential elements in ensuring the necessary referrals at the appropriate times56.
The study reports that FHS coverage was directly linked to the low municipal COVID-19 mortality rate, which supports the equitable application of PHC, given that this coverage is higher in smaller rural communities with infrastructure deficits and limited access to goods and services. Furthermore, they reinforce that, despite the difficulties faced in the North and Northeast regions, the active mobilization of community members and social support were essential for containing the pandemic. The high rates of social isolation during the first wave of the pandemic and the coordination between state governments for the sharing and implementation of health surveillance measures are clear examples of the effectiveness of the health actions carried out by PHC professionals57.
In the face of challenging situations that have a strong social, economic, and political impact, such as pandemics, the increase in negative psychological symptoms is intrinsically linked to profound changes in individuals' lifestyles and perceptions, and an increase in psychological disorders resulting from this experience is to be expected. In addition, the work overload faced by healthcare professionals during the pandemic may have been another factor in the emergence or worsening of mental disorders among these professionals58.
Given the central importance of PHC in tackling the COVID-19 virus, there has been a notable increase in the emotional strain and exhaustion of professionals in the face of the crisis, resulting in symptoms of anxiety, poor sleep quality, fear, and insecurity about infection in themselves and those close to them59. In this sense, there is a need to implement mental health care strategies for workers, as provided for in the National Policy on Worker Health, established in 2012, seeking to restore the work environment and promote psychological support for health professionals, with direct positive effects on the quality of care provided to the population60.
Scientific Approaches in the Study of Public Health
Thematic category 4 accounts for 20.08% of the text segments and includes the following significant words: qualitative, interview, quantitative, questionnaire, Bardin, and exploratory. The study of collective health can be conducted through interdisciplinary approaches that examine the social, economic, cultural, and environmental determinants of population health. In the context of PHC, these approaches can be applied to promote equity in access to care by implementing preventive medicine, longitudinal monitoring of chronic conditions, and promoting healthy habits.
Qualitative methods in public health enable us to understand not only how interventions are experienced but also the factors that influence individuals' participation or non-participation, and the possibilities for improving these actions. By clarifying the barriers and facilitators of care, qualitative health research produces detailed knowledge of strategies to make services more responsive to the populations they serve. In this sense, participatory, community-based, and artistic qualitative studies are fundamental tools for ensuring ethical and democratic engagement and preventing the marginalization of young people and other non-majority groups61.
After consulting the virtual library collection of the Postgraduate Program, the main topics chosen can be identified as: chronic noncommunicable diseases (CNCDs), with emphasis on systemic arterial hypertension (SAH), diabetes mellitus (DM), breast cancer and prostate cancer, COVID-19, nutrition, syphilis, and Autism Spectrum Disorder (ASD). Among methodological approaches, the qualitative approach was most prevalent (27%), followed by the quantitative approach (14.1%).
In the field of scientific research related to chronic noncommunicable diseases (NCDs), there is a predominance of studies addressing risk factors, treatment adherence, and the physical repercussions of these conditions, often developed from regional perspectives based on specific population analyses from different locations. The regionalized approach is relevant because it contributes significantly to the strategic direction and organization of PHC, especially regarding screening and comprehensive care for individuals in this epidemiological context.
In addition, discussions focused on neoplasms with high prevalence and relevance in the Brazilian context, such as breast, cervical, and prostate cancers, highlight the importance of adequate follow-up of patients affected by these conditions. The studies analyzed demonstrate the positive effects of this continuous surveillance on the clinical evolution of cases and provide an essential epidemiological framework to support the organization and strengthening of the health system in the context of oncological follow-up. In this sense, the strategic role of PHC is reinforced by its contribution to the prevention and control of diseases associated with these conditions, thereby promoting comprehensive and longitudinal care.
A substantial body of scientific publications on the COVID-19 pandemic and its effects on PHC has been reported, including studies involving both health professionals and service users. These investigations focused primarily on mental health-related factors, such as stressful scenarios, and on the direct and indirect impacts on PHC functioning as a gateway to the health system.
The incorporation of findings on the impacts of the COVID-19 pandemic on PHC highlights the need to strengthen the resilience of services, the mental health of workers, and the system's response capacity in the face of health emergencies. In this way, regional scientific productions support the PNAB by providing contextualized evidence that guides local planning, broadens the scope of health promotion, and consolidates the role of PHC as a structuring axis of the SUS.
A limiting factor of the study was the restriction to analyzing abstracts, which may have limited the depth of the discussion and access to detailed data that would be present in the full text of the theses and dissertations. In addition, relevant literature is scarce in languages other than Brazilian Portuguese, which made it difficult to compare and analyze international PHC models. Furthermore, the research was restricted to the North and Northeast regions of Brazil, which limits the generalization of the results to the other areas of the country, whose socioeconomic and infrastructure realities may differ substantially.
Conclusion
The analysis of the abstracts of dissertations and theses produced between 2020 and 2024 in graduate programs in Public Health and Family Health in the North and Northeast regions highlights the significant contribution of scientific production to strengthening the National Primary Care Policy (PNAB) and promoting health in the SUS. The predominance of qualitative research, with an interdisciplinary and territorialized approach, demonstrates the relevance of social, economic, cultural, and environmental determinants in the organization of PHC actions and confirms the strategic role of regional graduate studies in producing knowledge applicable to local realities.
These productions contribute to improving equity, comprehensiveness of care, and the qualification of surveillance, prevention, and longitudinal follow-up practices, including dimensions related to chronic non-communicable diseases and oncological conditions. Convergingly, studies show that the implementation of the PNAB has driven important advances in the organization and strengthening of the SUS, by prioritizing primary care as the basis for comprehensive care, expanding access, strengthening preventive practices, and reducing avoidable hospitalizations, especially in vulnerable regions and among at-risk social groups.
By mapping, for the first time, the thematic direction of academic productions from the North/Northeast on the PNAB, this study fills a regional gap and reinforces the importance of interdisciplinary work for understanding the complexity that permeates PHC. The findings demonstrate that the PNAB plays a central role in the coordination of care, the comprehensiveness of actions, and the promotion of equity, consolidating PHC as the main space for the realization of health promotion in the SUS.
Furthermore, there is a need to expand research that considers other Brazilian regions and engages with international literature, in order to broaden the understanding of the effects of the PNAB (National Primary Care Policy) on the organization of the health system. Strengthening research focused on territorial realities, social determinants, and care practices remains essential to improve responses to the population's needs and consolidate the PNAB as a structuring axis for a more effective, participatory public health system that promotes collective well-being.
Authors Contributions
Study design: Luciana Dantas Farias de Andrade; Stephany Raquel Leonço Mota. Data collection: Luciana Dantas Farias de Andrade; Stephany Raquel Leonço Mota. Data analysis and interpretation: Luciana Dantas Farias de Andrade; Stephany Raquel Leonço Mota. Manuscript writing: Luciana Dantas Farias de Andrade; Stephany Raquel Leonço Mota. Critical review of the manuscript: Luciana Dantas Farias de Andrade; Crisalda Eslita Silva Silveira; Marcela Samara Lira da Silva; Maria Clara Soares Dantas. Approval of the final version of the text: Luciana Dantas Farias de Andrade; Stephany Raquel Leonço Mota; Crisalda Eslita Silva Silveira; Marcela Samara Lira da Silva; Maria Clara Soares Dantas.
Conflict of interest
The authors have declared that there is no conflict of interest.
References
1. Pase HL, Patella APD, Santos ER. O pacto federativo e a implementação da política pública de saúde no Brasil. Caderno CRH [Internet]. 2023 [cited 2025 July 05];36:e023013. DOI: https://doi.org/10.9771/ccrh.v36i0.31794
2. Flauzino JGP, Angelini CFR. O direito à saúde e a legislação brasileira: uma análise a partir da Constituição Federal de 1988 e lei orgânica do Sistema Único de Saúde (SUS). Revista Eletrônica Acervo Saúde [Internet]. 2022 [cited 2025 Mar 27];15(3):e9957. DOI: https://doi.org/10.25248/reas.e9957.2022
3. Valerio FR, Silva ACR, Silva EH, Storck IJV, Branco FAC, Silva GC, Carvalho RCL, Azevedo MT. Universalidade de acesso aos serviços públicos no Brasil: uma revisão integrativa. Centro de Pesquisas Avançadas em Qualidade de Vida [Internet]. 2024 [cited 2025 Mar 27];16(2). Available from: https://revista.cpaqv.org/index.php/CPAQV/article/view/2028/1487
4. Ramos MS. A dicotomia integralidade versus fragmentação no Sistema Único de Saúde - SUS: um olhar a partir da governança [dissertação]. Foz do Iguaçu (PR): Universidade Federal da Integração Latino-Americana. 2024 [cited 2025 Mar 27]. Available from: https://dspace.unila.edu.br/handle/123456789/8836
5. Kessler M, Thumé E, Marmot M, Macinko J, Facchini LA, Nedel FB, Wachs LS, Volz PM, Oliveira C. Family Health Strategy, Primary Health Care, and social inequalities in mortality among older adults in Bagé, Southern Brazil. Am J Public Health. 2021 [cited 2025 Mar 27];111(5):927-936. DOI: https://doi.org/10.2105/AJPH.2020.306146
6. Sellera PEG, Silva MRM, Mendonça AVM, Ginani VC, Sousa MF. Incentivo de capitação ponderada (Programa Previne Brasil): impactos na evolução do cadastro populacional na APS. Ciênc saúde coletiva [Internet]. 2023 [cited 2025 July 05];28(9):2743–50. DOI: https://doi.org/10.1590/1413-81232023289.20142022
7. Silva GCGV, Silva MAM, Nogueira PP, Barbosa OLC. Desafios da Política Nacional de Atenção Básica à Saúde. Revista Pró-UniverSUS. 2021 [cited 2025 Mar 27];12(1):60-5. Available from: https://editora.univassouras.edu.br/index.php/RPU/article/view/2621/1591
8. Carmo ADN, Silva SLA, Campos EMS. Análise temporal de indicadores da Estratégia Saúde da Família sob o olhar da Política Nacional da Atenção Básica. Cad Saúde Pública [Internet]. 2023 [cited 2025 Mar 27];39(8):e00042523. DOI: https://doi.org/10.1590/0102-311XPT042523
9. Powell M, Williams I. What is a ‘National’ ‘Health’ ‘Service’? A keyword analysis of policy documents leading to the formation of the UK NHS. Health Economics, Policy and Law. 2024 [cited 2025 Mar 31];19(3):323–36. DOI: https://doi.org/10.1017/S1744133124000057
10. Keith RM. Universal health coverage by 2030, or the right to health? the continued relevance of the Alma Ata principles of voice and equity, through an intersectoral approach, to reducing global inequalities [thesis]. London: University of Westminster. 2021 [cited 2025 Mar 31]. DOI: https://doi.org/10.34737/v6w01
11. Almeida PF, Giovanella L, Schenkman S, Franco CM, Duarte PO, Houghton N, Báscolo E, Bousquat A. Perspectivas para las políticas públicas de Atención Primaria en Salud en Suramérica. Cien Saude Colet. 2024 [cited 2025 July 05];29(7):e03792024. DOI: https://doi.org/10.1590/1413-81232024297.03792024
12. Maceira D, Quintero REP, Suarez P, Peña LVP. Primary health care as a tool to promote equity and sustainability; a review of Latin American and Caribbean literature. Int J Equity Health [Internet]. 2024 [cited 2025 Nov 13];23(91). DOI: https://doi.org/10.1186/s12939-024-02149-9
13. Giovanella L, Vega R, Tejerina-Silva H, Acosta-Ramirez N, Parada-Lezcano M, Ríos G, Iturrieta D, Almeida PF, FEO O. ¿Es la atención primaria de salud integral parte de la respuesta a la pandemia de Covid-19 en Latinoamérica?. Trab educ saúde [Internet]. 2021 [cited 2025 Nov 13];19:e00310142. DOI: https://doi.org/10.1590/1981-7746-sol00310
14. Almeida PF, Giovanella L, Schenkman S, Franco CM, Duarte PO, Houghton N, Báscolo E, Bousquat A. Perspectivas para las políticas públicas de Atención Primaria en Salud en Suramérica. Ciênc saúde coletiva [Internet]. 2024 [cited 2025 Nov 13];29(7):e03792024. DOI: https://doi.org/10.1590/1413-81232024297.03792024
15. Wenceslau LD, Sarti TD, Trindade TG. Reflexões e propostas para a estruturação de programas de mestrado em medicina de família e comunidade no Brasil. Ciênc Saúde Colet [Internet]. 2020 [cited 2025 Apr 30];25(4):1281–92. DOI: https://doi.org/10.1590/1413-81232020254.29802019
16. BRASIL. Lei n° 13.709, de 14 de agosto de 2018. Lei Geral de Proteção de Dados [Internet]. Diário Oficial da União 14 ago 2018 [cited 2025 Nov 10]. Available from: https://www.planalto.gov.br/ccivil_03/_ato2015-2018/2018/lei/l13709.htm
17. Cardoso MRG, Oliveira GS, Ghelli KGM. Análise de conteúdo: uma metodologia de pesquisa qualitativa. Cadernos da Fucamp [Internet]. 2021 [cited 2025 Mar 11];20(43):98-111. Available from: https://revistas.fucamp.edu.br/index.php/cadernos/article/view/2347
18. Bardin L. Análise de Conteúdo. 1° ed. São Paulo: Edições 70; 2016 [cited 2025 Mar 11].
19. Souza JR, Santos SCM. Análise de conteúdo em pesquisa qualitativa: modo de pensar e de fazer. Pesquisa e Debate em Educação [Internet]. 2020 [cited 2025 Mar 11];10(2):1396-1416. DOI: https://doi.org/10.34019/2237-9444.2020.v10.31559
20. Medeiros FAB, Santos JMO, Mota HCN, Andrade IGM. O Iramuteq como ferramenta no processamento de dados em pesquisa qualitativa. Diálogos em Saúde Pública [Internet]. 2022 [cited 2025 Mar 11];1(2):000026. Available from: https://revistadialogos.saude.rn.gov.br/index.php/EPS/article/view/26/17
21. Silva S, Ribeiro EAW. The IRAMUTEQ software as a methodological tool for qualitative analysis in research in professional and technological education. Br. J. Ed., Tech. Soc. [Internet]. 2021 [cited 2025 July 5];14(2):275-84. DOI: https://doi.org/10.14571/brajets.v14.n2.275-284
22. Neto WAF, Júnior JDC, Ziede MKL, Bresolin P, Fernandes RAC, Bastos PV, Carvalho RS, Real LC. Programa saúde com agente: reflexões de educandos sobre metodologias ativas na educação a distância. RENOTE [Internet]. 2024 [cited 2025 Apr 30];22(2):12-24. Available from: https://seer.ufrgs.br/index.php/renote/article/view/142531/93047
23. Silva LS, Viegas SM da F, Nascimento LC do, Menezes C, Martins JRT, Potrich T. Universalidade do acesso e acessibilidade no quotidiano da atenção primária: vivências de usuários do SUS. Rev enferm Cent-Oeste Min [Internet]. 2020 [cited 2025 Mar 27];10:e3575. DOI: https://doi.org/10.19175/recom.v10i0.3575
24. Franco ACR, Penido CMF. Coprodução de autonomia na Atenção Primária à Saúde . Saude soc [Internet]. 2025 [cited 2025 July 05];34(1):e240363pt. DOI: https://doi.org/10.1590/S0104-12902025240363pt
25. Santos GXG, Silva SP, Nascimento JWA, Coutinho DJG. Impactos da política nacional de atenção básica nas taxas de mortalidade infantil sob a ótica da estratégia de saúde da família. REAEnf [Internet]. 2020 [cited 2025 Mar 27];7:e5719. DOI: https://doi.org/10.25248/REAenf.e5719.2020
26. Pitta SCBS. Saúde Materno-Infantil: saberes e práticas do agente comunitário de saúde na visita domiciliar no âmbito do programa de Agentes Comunitários de Saúde. Fortaleza. Dissertação [Mestrado Profissional em Avaliação de Políticas Públicas] - Universidade Federal do Ceará; 2025. Availabe from: https://repositorio.ufc.br/bitstream/riufc/82733/2/2025_dis_scbspitta.pdf
27. Pasklan ANP, Queiroz RCS, Rocha TAH, Silva NC, Tonello AS, Vissoci JRN, Tomasi E, Thumé E, Staton C, Thomaz EBAF. Análise espacial da qualidade dos serviços de Atenção Primária à Saúde na redução da mortalidade infantil. Ciênc saúde coletiva [Internet]. 2021 [cited 2025 Nov 12];26(12):6247–58. DOI: https://doi.org/10.1590/1413-812320212612.24732020
28. Holanda WTG, Oliveira SB, Sanchez MN. Aspectos diferenciais do acesso e qualidade da atenção primária à saúde no alcance da cobertura vacinal de influenza. Ciênc saúde coletiva [Internet]. 2022 [cited 13 Nov 2025];27(4):1679-94. DOI: https://doi.org/10.1590/1413-81232022274.03472021.
29. Santos MTS, Carvalho TA, Santos TRM, Brito MJA, Holanda DAM, Silva MSF, Andrade ES, Cartaxo LS, Rodrigues ARGM. Importance of the CHA's work in vaccination monitoring actions in children under 5 years of age: integrative review. RSD [Internet]. 2023 [cited 2025 Nov 13];12(2):e9212239981. DOI: http://dx.doi.org/10.33448/rsd-v12i2.39981
30. Rocha ESC, Toledo NN, Pina RMP, Fausto MCR, D’Viana AL, Lacerda RA. Primary Health Care attributes in the context of indigenous health. Revista Brasileira de Enfermagem. 2020 [cited 2025 Mar 27];73(5):e20190641. DOI: http://dx.doi.org/10.1590/0034-7167-2019-0641
31. Gontijo LA, Silva BM, Viegas SMF. Atenção à saúde de pessoas em situação de rua no cotidiano da atenção primária: scoping review. Saúde em Debate [Internet]. 2023 [cited 2025 Nov 12];47(137):316-32. DOI: https://doi.org/10.1590/0103-1104202313722.
32. Mendes AM,, Leite MS, Langdon EJ, Grisotti M. O desafio da atenção primária na saúde indígena no Brasil. Rev Panam Salud Publica [Internet]. 2018 [cited 2025 Nov 12];42:e184. DOI: https://doi.org/10.26633/RPSP.2018.184
33. Rocha ESC, Toledo N das N, Pina RMP, Fausto MCR, D’Viana AL, Lacerda RA. Primary Health Care attributes in the context of indigenous health. Rev Bras Enferm [Internet]. 2020;73(5):e20190641. DOI: https://doi.org/10.1590/0034-7167-2019-0641
34. Lima JG, Giovanella L, Fausto MCR, Mendonça MHM. Organização da Atenção Primária à Saúde em municípios rurais remotos do oeste do Pará. Saúde em Debate [Internet]. [cited 2025 Nov 12];47(139):858-77. DOI: https://doi.org/10.1590/0103-1104202313910
35. Rodrigues KV, Almeida PF, Cabral LMS, Fausto MCR. Organização da Atenção Primária à Saúde em um município rural remoto do norte do Brasil. Saúde debate [Internet]. 2021 [cited 2025 Nov 12];45(131):998–1016. DOI: https://doi.org/10.1590/0103-1104202113105
36. Barbosa TMS, da Silva FS, da Silva GJ, Miranda LVM de C, Maslinkiewicz A, Alves AP da P, de Morais JCL, Souza CR da S. Abordagem multidisciplinar na Atenção Primária à Saúde: potencializando a colaboração para cuidados de qualidade. Rev Contemp [Internet]. 2023 [cited 2025 Apr 01];3(9):14675-87. DOI: https://doi.org/10.56083/RCV3N9-066
37. Vendruscolo C, Silva KJ, Araújo JAD, Weber ML. Educação permanente e sua interface com melhores práticas em enfermagem na atenção primária à saúde. Cogitare Enfermagem [Internet]. 2021 [cited 2025 Apr 01];26:e72725. DOI: https://doi.org/10.5380/ce.v26i0.72725
38. Melo DFC, Ribeiro APTB, Rodrigues RS, Rodrigues VG, Neto FRGX, Cavalcante RS, Andrade MG, Albuquerque IMN, Ribeiro MA, Holanda DXT. Educação permanente em saúde na Atenção Primária à Saúde: um desafio para a construção de práticas efetivas e sustentáveis. ARE [Internet]. 2025 [cited 2025 Nov 12];7(6):35098-126. DOI: https://doi.org/10.56238/arev7n6-347
39. Gonçalves DF, Figueira Y, Menezes CN, Fontoura VM, Filho JAS, Cupolillo AV, França CDMM, Schaefer FM. Importância da atenção primária para a prevenção de doenças não transmissíveis. Revista Foco [Internet]. 2024 [cited 2025 Apr 01];17(8):e6033. DOI: https://doi.org/10.54751/revistafoco.v17n8-149
40. Organização para a Cooperação e Desenvolvimento Econômico. Estudo da OCDE da Atenção Primária à Saúde no Brasil. Paris: OECD Publishing; 2021 [cited 2025 Apr 01]. DOI: https://doi.org/10.1787/9bf007f4-pt
41. Andrade MG, Melo DFC, Machado ALLB, Pereira MLM, Campos GTTP, Melo FMS, Lima LXSM, Feitosa ALM, Rodrigues RS, Costa NF. Câncer de colo do útero: estratégias de controle na Atenção Primária a Saúde. Revista Eletrônica Acervo Saúde [Internet]. 2023 [cited 2025 Apr 01];23(8):e13354. DOI: https://doi.org/10.25248/REAS.e13354.2023
42. Silva DCB, Garnelo L, Herkrath FJ. Barriers to access the pap smear test for cervical cancer screening in rural riverside populations covered by a fluvial Primary Healthcare Team in the Amazon. Int. J. Environ. Res. Public Health. 2022 [cited 2025 Nov 12];19(7):4193. DOI: https://doi.org/10.3390/ijerph19074193
43. Reis RS, Lima FCS, Silva DHN, Cavalcante JPF, Corrêa FM, Santos YRP, Scaff AJM. Infecção por HPV e controle do câncer no Brasil: o importante papel da vacinação. Rev Bras Cancerol [Internet]. 2025 [cited 2025 Nov 12];71(1):e–164928. DOI: https://doi.org/10.32635/2176-9745.RBC.2025v71n1.4928
44. Freitas EGS, Carvalho BF, Sampaio MFB, Luz VEB, Vasconcelos AF. Mortality from cervical cancer in brazilian regions: an ecological study. RSD [Internet]. 2024 Jan. 23 [cited 2025 Nov 12];13(1):e10713144848. DOI: https://doi.org/10.33448/rsd-v13i1.44848
45. Guedes TRON, Santos ICPAM, Filha JAP, Espinar RMS, Souza RFP, Cavalcante ER, Veiga AS, Silva IM, SCHWEICKARDT JC. Estratégias educativas para aumentar a adesão ao exame papanicolau: a experiência da UBSF O-16, Manaus-AM. Saúde Redes [Internet]. 2021 [cited 2025 Nov 12];7(2):61-7. Availabe from https://revista.redeunida.org.br/index.php/rede-unida/article/view/3582/706
46. Pedreira VMR, Santos RLO, Rocha ACS, Kasburg SN, Gonçalves JR, Venancio TNV, Rufino LRMC, Junior WPC. A relação entre o câncer de colo de útero e o HPV: uma análise bibliográfica. Brazilian Journal of Health Review [Internet]. 2023 [cited 2025 Apr 1];6(5):20898-20911. DOI: https://doi.org/10.34119/bjhrv6n5-120
47. Freitas MCA, Dutra VA, Graça IVO, Batalha G. Epidemiologia do câncer de colo de útero no norte do Brasil entre 2011 e 2021: um estudo ecológico. Brazilian Journal of Health Review. 2024 [cited 2025 Nov 12];7(4):01-14. DOI: https://doi.org/10.34119/bjhrv7n4-434
48. Brito GEG, Forte FDS, Freire JCG, Moreira LB, Paredes SO, Silva SLA. Articulação entre a EqSF/AB e o NASF/AB e sua influência na produção do cuidado no contexto da Atenção Primária à Saúde. Ciênc saúde coletiva [Internet]. 2022 [cited 2025 Nov 12];27(6):2495–508. DOI: https://doi.org/10.1590/1413-81232022276.03942021
49. Dimenstein M, Macedo JP, Silva BÍBM. Capacidade de resposta do NASF em saúde mental. Physis [Internet]. 2023 [cited 2025 Nov 12];33:e33017. DOI: https://doi.org/10.1590/S0103-7331202333017
50. Bispo, José Patrício e Almeida, Erika Rodrigues. Equipes multiprofissionais (eMulti): potencialidades e desafios para a ampliação da atenção primária à saúde no Brasil. Cadernos de Saúde Pública [online]. v. 39, n. 10 [cited 2025 Nov 11];39(10):e00120123. DOI: https://doi.org/10.1590/0102-311XPT120123
51. Weiler AB, Camargo MEB, Burg MR. Percepção dos gestores sobre o impacto da Covid-19 nos serviços da atenção primária à saúde. Revista Científica Multidisciplinar [Internet]. 2022 [cited 2025 Abr 03];3(8):e381794. DOI: https://doi.org/10.47820/recima21.v3i8.1794
52. Santos HLPC, Prado NMBL, Santos LHPE, Maciel FBM, Pereira LV, Teixeira CF. Processo de organização do trabalho dos Núcleos Ampliados de Saúde da Família e Atenção Básica durante a pandemia da Covid-19 no Brasil. Saúde debate [Internet]. 2023[cited 2025 Nov 10];47(139):978–92. DOI: https://doi.org/10.1590/0103-1104202313918
53. Santana MM, Medeiros KR, Monken M. Processo de trabalho da Estratégia Saúde da Família na pandemia no Recife-PE: singularidades socioespaciais. Trab educ saúde [Internet]. 2022 [cited 2025 Nov 10];20:e00154167. DOI: https://doi.org/10.1590/1981-7746-ojs00154
54. Silva NRB. O processo de trabalho em saúde do NASF na pandemia da Covid-19: mudanças e repercussões. João Pessoa. Dissertação [Mestrado em Saúde Coletiva] - Universidade Federal da Paraíba; 2023. https://repositorio.ufpb.br/jspui/bitstream/123456789/34224/1/NaraRaquelBarbosaDaSilva_Dissert.pdf
55. Giovanella L, Martufi V, Mendoza DCR, Mendonça MHM de, Bousquat A, Aquino R, Medina MG. A contribuição da Atenção Primária à Saúde na rede SUS de enfrentamento à Covid-19. Saúde em Debate [Internet]. 2020 [cited 2025 Apr 03];44(esp4):161–76. DOI: https://doi.org/10.1590/0103-11042020E410
56. Corrêa APV, Magno GD, Rodrigues RCP, Cano RN, Medina IML, Nieto CA, Uehara SCSA. Diferenças regionais na reorganização da Atenção Primária à Saúde no contexto da pandemia de Covid-19 no Brasil. Cien Saude Colet [Internet] 2024 [cited 2025 Nov 10]. DOI: https://doi.org/10.1590/1413-812320253012.06882024
57. Schenkman S, Bousquat AEM, Facchini LA, Gil CRR, Giovanella L. Performance patterns of primary health care in the face of COVID-19 in Brazil: characteristics and contrasts. Cad. Saúde Pública. 2023 [cited 2025 Nov 10];39(8):e00009123. DOI: https://doi.org/10.1590/0102-311XEN009123
58. Vasconcellos DRF. Sintomas emocionais negativos entre discentes e docentes das instituições de ensino superior no contexto da pandemia de Covid-19. Vitória da Conquista. Dissertação [Mestrado em Saúde Coletiva] - Universidade Federal da Bahia; 2023. Available from: https://repositorio.ufba.br/bitstream/ri/39300/1/DISSERTAÇÃO%20DANIELE%20FRÓES%20-%20FINAL%20com%20ficha%20cat%20e%20assinaturas%2022%2003%2024.pdf
59. Dantas ESO. Saúde mental dos profissionais de saúde no Brasil no contexto da pandemia por Covid-19. Interface (Botucatu) [Internet]. 2021 [cited 2025 Apr 03];25(supl. 1):e200203. DOI: https://doi.org/10.1590/Interface.200203
60. Faria MGA, Silveira EA, Cabral GRFC, Silva RO, Daher DV, David HMSL. Saúde do trabalhador no contexto da estratégia de saúde da família: revisão integrativa de literatura. Esc Anna Nery [Internet]. 2020 [cited 2025 June 01];24(4):e20200027. DOI: https://doi.org/10.1590/2177-9465-EAN-2020-0027
61. Allen LP, Kelly C, Hatala AR. Answering tough questions: why is qualitative research essential for public health? Australian and New Zealand Journal of Public Health. 2024 [cited 2025 Nov 13];48(3). DOI: https://doi.org/10.1016/j.anzjph.2024.100157
Corresponding Author
Name: Stephany Raquel Leonço Mota
E-mail: stephanyleonco@gmail.com
The Author(s) 2026. This work is licensed under Creative Commons Attribution 4.0 International. License text for use: https://creativecommons.org/licenses/by/4.0/deed.pt_BR
 Português (Brasil)
Português (Brasil)  English
English  Español (España)
Español (España) 



















